University of Minnesota, Minneapolis, 55455, USA.
Curr Hematol Malig Rep. 2013 Sep;8(3):211-7. doi: 10.1007/s11899-013-0163-4.
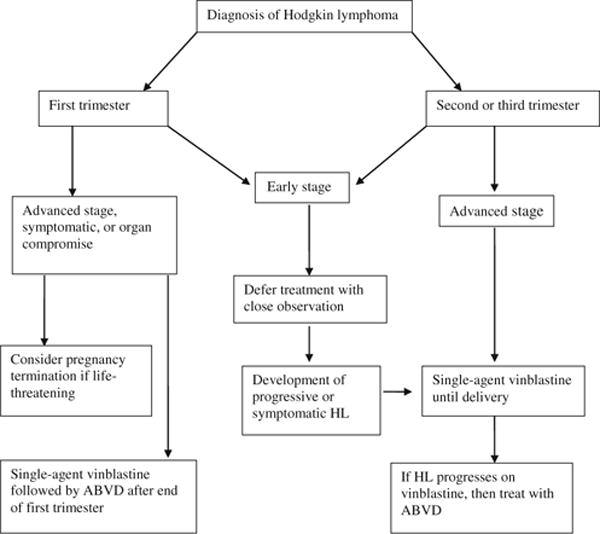
The peak incidence of Hodgkin lymphoma (HL) coincides with reproductive years, and as many as 3 % of all HL patients present with concurrent pregnancy. The management of a pregnant patient with HL requires a multidisciplinary approach combining expertise in medical oncology, high-risk obstetrics, and neonatology, as well as effective communication with the patient and her family. The goal is to optimize the mother's chance of a cure while allowing for delivery of a healthy child. A pregnant patient with HL should be staged by clinical examination and judicious use of non-radiation imaging such as ultrasound, balancing the need for accurate disease assessment with the need to minimize invasive procedures. The treatment strategy is individualized to the symptoms, lymphoma stage, gestational age and the patients' wishes. Therapeutic options include treatment deferral or single-agent vinblastine with reservation of multi-agent chemotherapy until the second or third trimester for the small minority of patients with aggressive clinical presentation.
霍奇金淋巴瘤 (HL) 的发病高峰与生育年龄相吻合,多达 3%的 HL 患者同时妊娠。HL 合并妊娠患者的管理需要多学科方法,结合医学肿瘤学、高危产科和新生儿学的专业知识,以及与患者及其家属的有效沟通。目标是优化母亲治愈的机会,同时确保生下健康的孩子。HL 合并妊娠的患者应通过临床检查和明智地使用非放射性成像(如超声)进行分期,在准确评估疾病的需求与尽量减少侵入性操作的需求之间取得平衡。治疗策略是根据症状、淋巴瘤分期、孕龄和患者的意愿个体化制定的。治疗选择包括延迟治疗或单药长春碱,对于少数临床表现侵袭性强的患者,保留多药化疗至妊娠中期或晚期。