Marinari Stefano, Manigrasso Maria Rosaria, De Benedetto Fernando
Pneumology Department, SS Annunziata Hospital, Chieti, Italy.
Multidiscip Respir Med. 2013 Jun 21;8(1):40. doi: 10.1186/2049-6958-8-40.
The protein-calorie malnutrition, resulting in muscle mass loss, frequently occurs in severe COPD patients with chronic respiratory failure (CRF), causing dyspnea, reduced exercise tolerance and impaired quality of life.The cause of this occurrence is an intake-output energy imbalance. A documented deficit of phosphocreatine and reduced mithocondrial energy production can contribute to this imbalance.Aim of this study is to verify whether a dietary supplementation with creatine and coenzyme Q10, important mitochondrial function factors, is able to influence this mechanism leading to a dyspnea reduction and improving exercise tolerance and quality of life.
55 COPD patients with chronic respiratory failure (in long term O2 therapy), in stable phase of the disease and without severe comorbidities were assigned (double-blind, randomized) to: group A (30 patients) with daily dietary supplementation with Creatine 340 mg + 320 mg Coenzyme Q-Ter (Eufortyn®, Scharper Therapeutics Srl) for 2 months whereas Group B (25 patients) received placebo.All patients continued the same diet, rehabilitation and therapy during the study. At recruitment (T0) and after 2 months (T1), patients were submitted to medical history, anthropometry (BMI), bioelectrical impedance, arterial blood gas analysis, evaluation of dyspnea (VAS, Borg, BDI, MRC) and functional independence (ADL), 6-minute walk test (6MWT) and quality of life questionnaire (SGRQ). At 6 months and 1 year, a telephone follow up was conducted on exacerbations number.
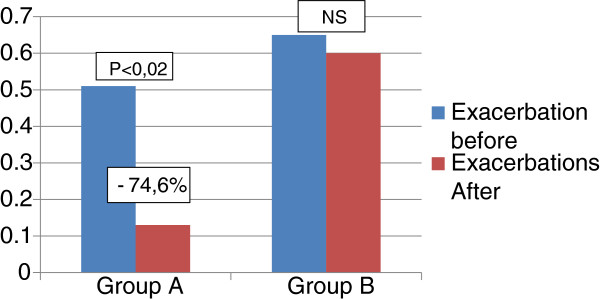
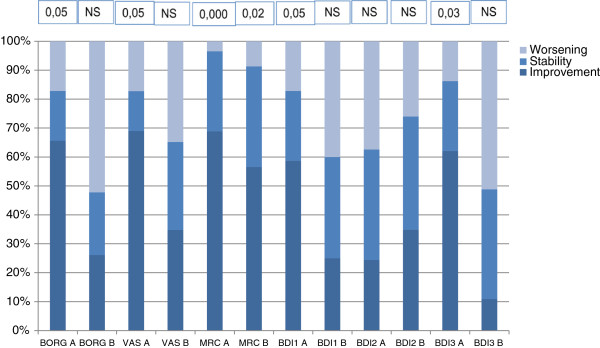
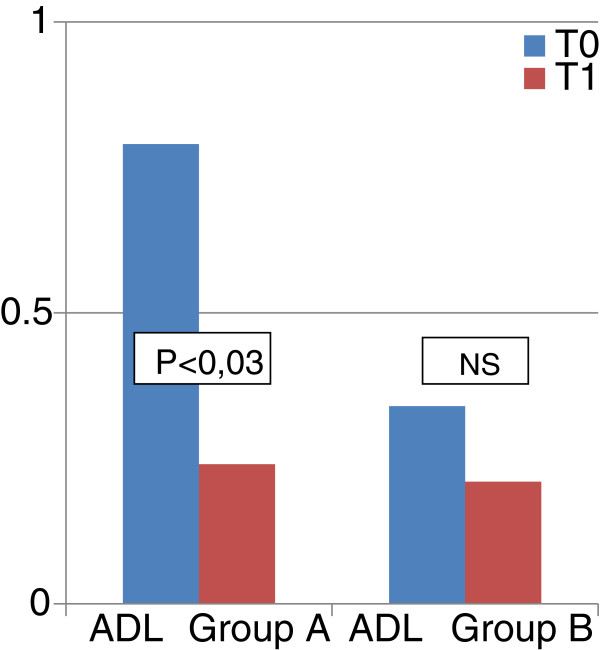
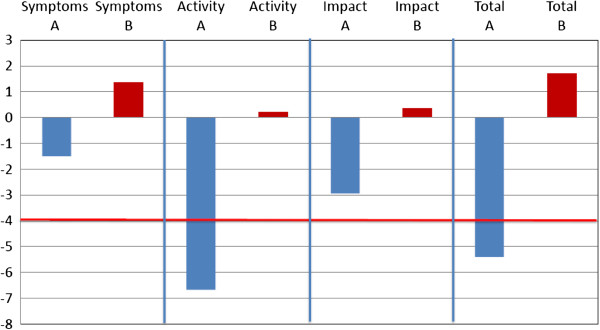
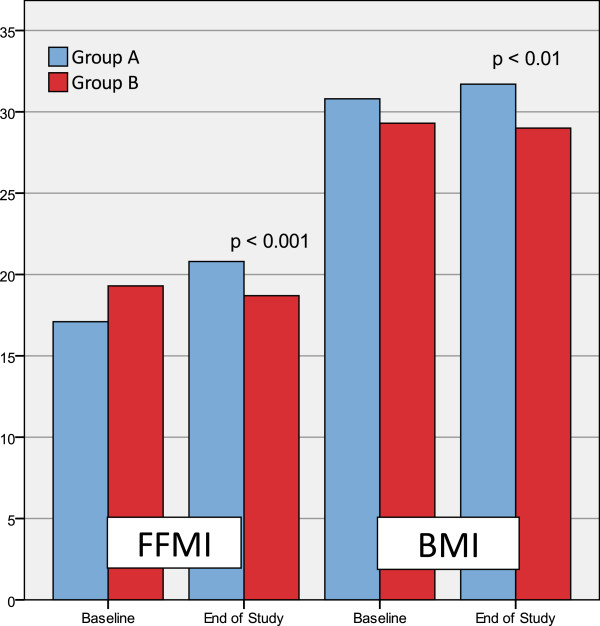
No significant difference was detected at baseline (T0) in the 2 groups. After 2 months of therapy (T1) the FFMI increased in the daily dietary supplementation group (+ 3.7 %) and decreased in the placebo group (- 0.6 %), resulting in a statistically significant (p < 0.001) treatment difference. Statistically significant treatment differences, favouring daily dietary supplementation group, were also seen for the 6MWT comparison. Group A patients also showed significant: 1) improvement in the degree of dyspnea (VAS: p < 0.05; Borg: p < 0.05; MRC: p < 0.001; BDI1: p < 0.05; BDI3: p < 0.03), and independence level in activities of daily living (p < 0.03); 2) improvement in quality of life in activity section (- 6.63 pt) and in total score (- 5.43 pt); 3) exacerbation number decrease (p < 0.02). No significant differences were found (end of study vs baseline) in group B.
The nutraceutical diet integration with Q-Ter and creatine, in COPD patients with CRF in O2TLT induced an increasing lean body mass and exercise tolerance, reducing dyspnea, quality of life and exacerbations. These results provide a first demonstration that acting on protein synthesis and muscular efficiency can significantly modify the systemic consequences of the disease.
蛋白质 - 热量营养不良导致肌肉量减少,在患有慢性呼吸衰竭(CRF)的重度慢性阻塞性肺疾病(COPD)患者中经常发生,会引起呼吸困难、运动耐力下降及生活质量受损。这种情况的发生原因是能量摄入与消耗不平衡。有记录表明磷酸肌酸缺乏和线粒体能量产生减少会导致这种不平衡。本研究的目的是验证补充肌酸和辅酶Q10(重要的线粒体功能因子)的饮食是否能够影响导致呼吸困难减轻、运动耐力和生活质量改善的这一机制。
55例患有慢性呼吸衰竭(长期接受氧气治疗)、处于疾病稳定期且无严重合并症的COPD患者被(双盲、随机)分配到:A组(30例患者),每天补充340毫克肌酸 + 320毫克辅酶Q - Ter(Eufortyn®,Scharper Therapeutics Srl),持续2个月;而B组(25例患者)接受安慰剂。在研究期间,所有患者继续相同的饮食、康复和治疗。在招募时(T0)和2个月后(T1),患者接受病史询问、人体测量(BMI)、生物电阻抗分析、动脉血气分析、呼吸困难评估(视觉模拟评分法、博格量表、呼吸困难指数、医学研究委员会量表)和功能独立性评估(日常生活活动能力量表)、6分钟步行试验(6MWT)以及生活质量问卷(圣乔治呼吸问卷)。在6个月和1年时,通过电话随访记录病情加重次数。
两组在基线(T0)时未检测到显著差异。治疗2个月后(T1),每日饮食补充组的去脂体重指数增加(+3.7%),安慰剂组下降(-0.6%),治疗差异具有统计学意义(p < 0.001)。在6MWT比较中也观察到有利于每日饮食补充组的具有统计学意义的治疗差异。A组患者还表现出显著:1)呼吸困难程度改善(视觉模拟评分法:p < 0.05;博格量表:p < 0.05;医学研究委员会量表:p < 0.001;呼吸困难指数1:p < 0.05;呼吸困难指数3:p < 0.03)以及日常生活活动独立性水平提高(p < 0.03);2)活动部分生活质量改善(-6.63分)和总分改善(-5.43分);3)病情加重次数减少(p < 0.02)。B组未发现显著差异(研究结束时与基线相比)。
对于接受氧气长期治疗的CRF合并COPD患者,添加辅酶Q - Ter和肌酸的营养饮食可增加瘦体重和运动耐力,减轻呼吸困难,改善生活质量并减少病情加重次数。这些结果首次证明作用于蛋白质合成和肌肉效率可显著改变该疾病的全身影响。