Department of Medical Physics, Memorial Sloan-Kettering Cancer Center, New York, New York.
Department of Medical Physics, Memorial Sloan-Kettering Cancer Center, New York, New York.
Int J Radiat Oncol Biol Phys. 2014 Feb 1;88(2):446-52. doi: 10.1016/j.ijrobp.2013.10.038. Epub 2013 Dec 5.
We hypothesized that a treatment planning technique that incorporates predicted lung tumor regression into optimization, predictive treatment planning (PTP), could allow dose escalation to the residual tumor while maintaining coverage of the initial target without increasing dose to surrounding organs at risk (OARs).
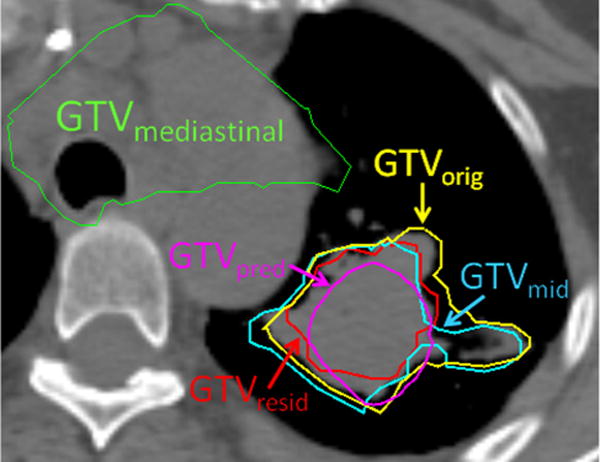
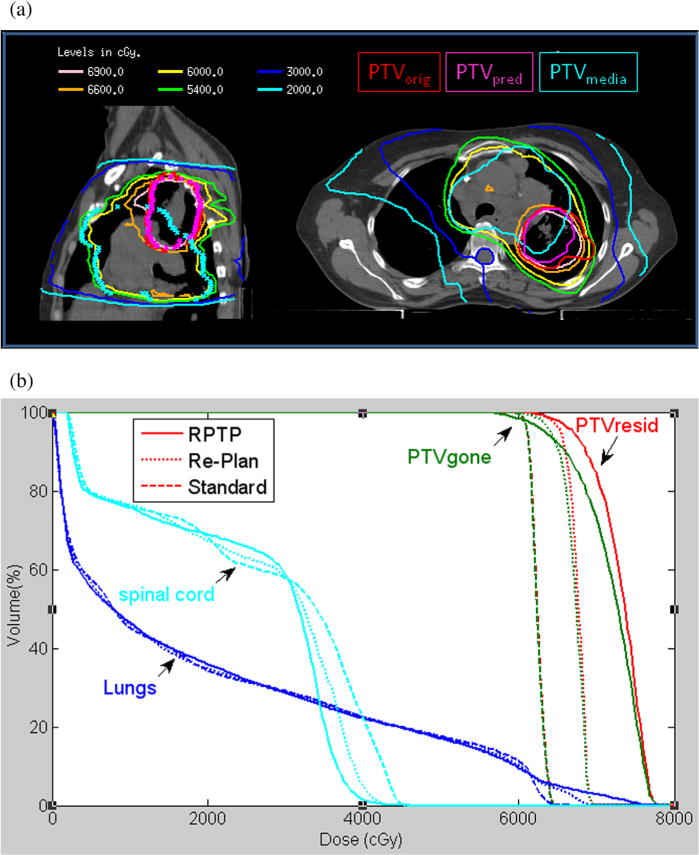
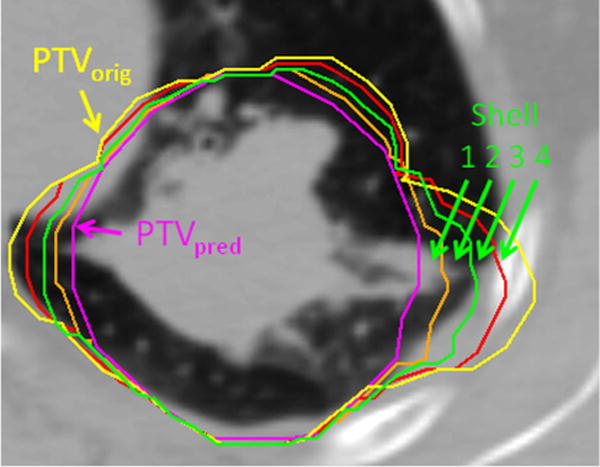
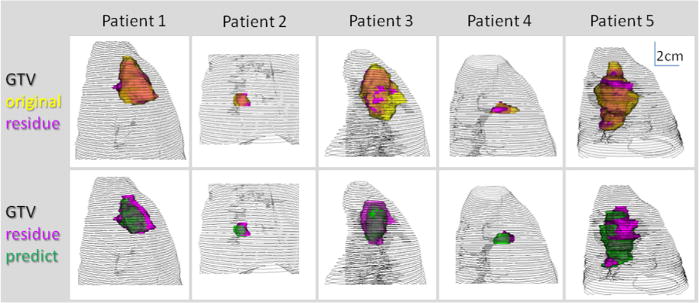
We created a model to estimate the geometric presence of residual tumors after radiation therapy using planning computed tomography (CT) and weekly cone beam CT scans of 5 lung cancer patients. For planning purposes, we modeled the dynamic process of tumor shrinkage by morphing the original planning target volume (PTVorig) in 3 equispaced steps to the predicted residue (PTVpred). Patients were treated with a uniform prescription dose to PTVorig. By contrast, PTP optimization started with the same prescription dose to PTVorig but linearly increased the dose at each step, until reaching the highest dose achievable to PTVpred consistent with OAR limits. This method is compared with midcourse adaptive replanning.
Initial parenchymal gross tumor volume (GTV) ranged from 3.6 to 186.5 cm(3). On average, the primary GTV and PTV decreased by 39% and 27%, respectively, at the end of treatment. The PTP approach gave PTVorig at least the prescription dose, and it increased the mean dose of the true residual tumor by an average of 6.0 Gy above the adaptive approach.
PTP, incorporating a tumor regression model from the start, represents a new approach to increase tumor dose without increasing toxicities, and reduce clinical workload compared with the adaptive approach, although model verification using per-patient midcourse imaging would be prudent.
我们假设一种治疗计划技术,即将预测的肺肿瘤退缩纳入优化过程中,即预测性治疗计划(PTP),可以在不增加周围危及器官(OAR)剂量的情况下,将剂量递送至残留肿瘤,同时保持初始靶区的覆盖范围。
我们创建了一个模型,使用计划计算机断层扫描(CT)和 5 例肺癌患者每周的锥形束 CT 扫描,来估计放射治疗后残留肿瘤的几何形态。为了规划目的,我们通过在 3 个等距步骤中将原始计划靶区(PTVorig)变形为预测的残留物(PTVpred),来模拟肿瘤收缩的动态过程。患者接受均匀处方剂量的 PTVorig 治疗。相比之下,PTP 优化从相同的 PTVorig 处方剂量开始,但在线性增加每个步骤的剂量,直到达到与 OAR 限制一致的 PTVpred 的最高可实现剂量。这种方法与中途自适应重新计划进行了比较。
初始实质大体肿瘤体积(GTV)范围为 3.6 至 186.5 cm³。平均而言,原发性 GTV 和 PTV 在治疗结束时分别减少了 39%和 27%。PTP 方法至少为 PTVorig 提供了处方剂量,并且比自适应方法平均增加了 6.0 Gy 的真实残留肿瘤的平均剂量。
从一开始就纳入肿瘤退缩模型的 PTP 代表了一种增加肿瘤剂量而不增加毒性的新方法,与自适应方法相比,减少了临床工作量,尽管使用每例患者的中途成像进行模型验证可能是谨慎的。