O'Neill William W, Schreiber Theodore, Wohns David H W, Rihal Charanjit, Naidu Srihari S, Civitello Andrew B, Dixon Simon R, Massaro Joseph M, Maini Brijeshwar, Ohman E Magnus
Henry Ford Hospital, Detroit, Michigan.
J Interv Cardiol. 2014 Feb;27(1):1-11. doi: 10.1111/joic.12080. Epub 2013 Dec 13.
To evaluate the periprocedural characteristics and outcomes of patients supported with Impella 2.5 prior to percutaneous coronary intervention (pre-PCI) versus those who received it after PCI (post-PCI) in the setting of cardiogenic shock (CS) complicating an acute myocardial infarction (AMI).
Early mechanical circulatory support may improve outcome in the setting of CS complicating an AMI. However, the optimal timing to initiate hemodynamic support has not been well characterized.
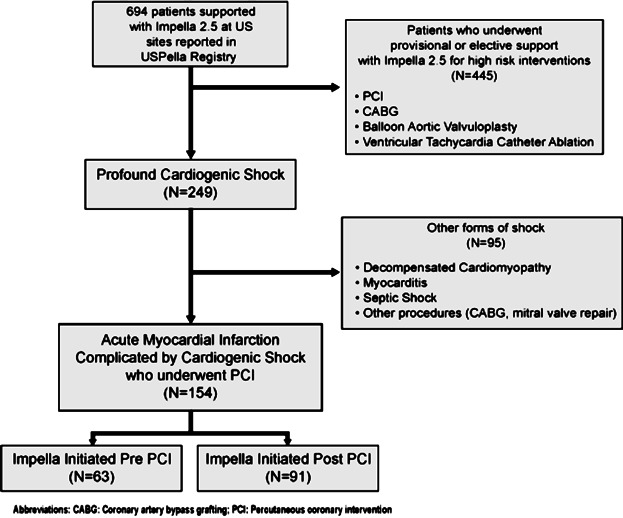
Data from 154 consecutive patients who underwent PCI and Impella 2.5 support from 38 US hospitals participating in the USpella Registry were included in our study. The primary end-point was survival to discharge. Secondary end-points included assessment of patients' hemodynamics and in-hospital complications. A multivariate regression model was used to identify independent predictors for mortality.
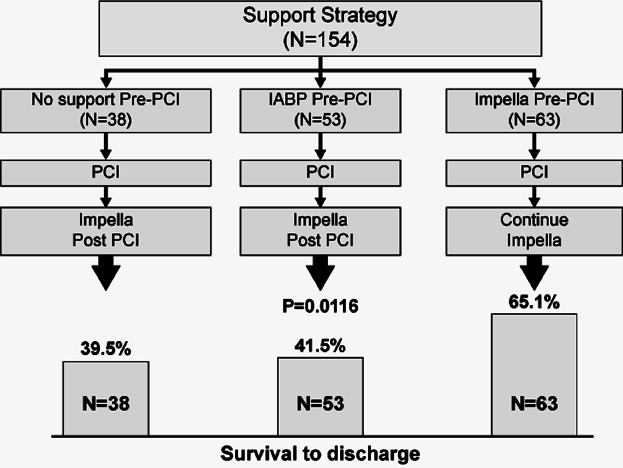
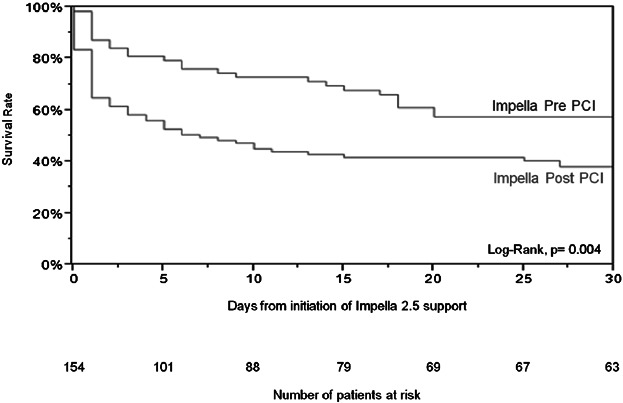
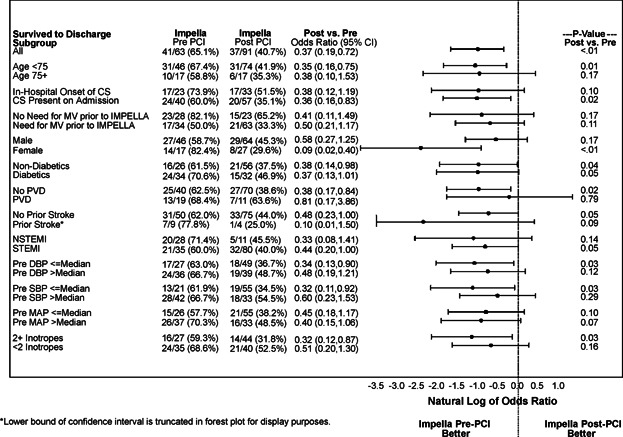
Both groups were comparable except for diabetes (P = 0.02), peripheral vascular disease (P = 0.008), chronic obstructive pulmonary disease (P = 0.05), and prior stroke (P = 0.04), all of which were more prevalent in the pre-PCI group. Patients in the pre-PCI group had more lesions (P = 0.006) and vessels (P = 0.01) treated. These patients had also significantly better survival to discharge compared to patients in the post-PCI group (65.1% vs.40.7%, P = 0.003). Survival remained favorable for the pre-PCI group after adjusting for potential confounding variables. Initiation of support prior to PCI with Impella 2.5 was an independent predictor of in-hospital survival (Odds ratio 0.37, 95% confidence interval: 0.17-0.79, P = 0.01) in multivariate analysis. The incidence of in-hospital complications included in the secondary end-point was similar between the 2 groups.
The results of our study suggest that early initiation of hemodynamic support prior to PCI with Impella 2.5 is associated with more complete revascularization and improved survival in the setting of refractory CS complicating an AMI.
评估在急性心肌梗死(AMI)并发心源性休克(CS)的情况下,经皮冠状动脉介入治疗(PCI)前接受Impella 2.5支持的患者与PCI后接受该支持的患者的围手术期特征和结局。
早期机械循环支持可能改善AMI并发CS患者的结局。然而,启动血流动力学支持的最佳时机尚未得到很好的界定。
我们的研究纳入了来自参与美国Impella注册研究的38家美国医院的154例连续接受PCI和Impella 2.5支持的患者的数据。主要终点是出院生存率。次要终点包括评估患者的血流动力学和院内并发症。使用多变量回归模型确定死亡率的独立预测因素。
除糖尿病(P = 0.02)、外周血管疾病(P = 0.008)、慢性阻塞性肺疾病(P = 0.05)和既往卒中(P = 0.04)外,两组具有可比性,所有这些在PCI前组中更为普遍。PCI前组治疗的病变(P = 0.006)和血管(P = 0.01)更多。与PCI后组患者相比,这些患者出院生存率也显著更高(65.1%对40.7%,P = 0.003)。在调整潜在混杂变量后,PCI前组的生存率仍然良好。在多变量分析中,PCI前使用Impella 2.5启动支持是院内生存的独立预测因素(比值比0.37,95%置信区间:0.17 - 0.79,P = 0.01)。次要终点中包括的院内并发症发生率在两组之间相似。
我们的研究结果表明,在AMI并发难治性CS的情况下,PCI前早期启动Impella 2.5进行血流动力学支持与更完全的心再灌注和改善的生存率相关。