McDonald Matthew R, Sathiyakumar Vasanth, Apfeld Jordan C, Hooe Benjamin, Ehrenfeld Jesse, Obremskey William T, Sethi Manish K
The Vanderbilt Orthopaedic Institute Center for Health Policy, Vanderbilt University, Suite 4200, South Tower, MCE, Nashville, TN, 37221, USA,
J Orthop Traumatol. 2014 Dec;15(4):255-8. doi: 10.1007/s10195-013-0280-9. Epub 2013 Dec 14.
Operative fixation of ankle fractures is common. However, as reimbursement plans evolve with the potential for bundled payments, it is critical that orthopedic surgeons better understand factors influencing the postoperative length of stay (LOS) in patients undergoing these procedures to negotiate appropriate reimbursement. We sought to identify factors influencing the postoperative LOS in patients with operatively treated ankle fractures.
Six hundred twenty-two patients with ankle fractures between January 1st, 2004 and December 31st, 2010 were identified retrospectively. Charts were reviewed for gender, length of operative procedure, method of fixation, American Society of Anesthesiologists (ASA) physical status score, medical comorbidities, and postoperative LOS. Both univariate and multivariate models were developed to determine predictors of patient LOS. Financial data for an average 24-h inpatient stay were obtained from financial services.
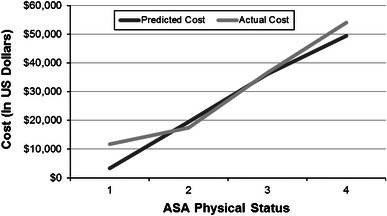
Six hundred twenty-two patients were included. In a linear regression analysis, a statistically significant relationship was demonstrated between ASA status and LOS (P < 0.001). Multiple regression analysis further characterized the relationship between ASA and LOS: a 1-U increase in ASA classification conferred a 3.42-day increase in LOS on average (P < 0.001). Based on an average per-day inpatient cost of $4,503, each unit increase in ASA status led to a $15,490 increase in cost.
Our study demonstrates that ASA status is a powerful predictor of LOS in patients undergoing operative fixation of ankle fractures. More complete understanding of these factors will lead to better risk adjustment models for measuring outcomes, determining fair reimbursement, and potential improvements to the efficiency of patient care.
Level III retrospective comparative study regressing length of stay with many variables, including ASA physical status.
踝关节骨折的手术固定很常见。然而,随着报销计划随着捆绑支付的可能性而演变,骨科医生更好地了解影响接受这些手术患者术后住院时间(LOS)的因素以协商适当的报销至关重要。我们试图确定影响接受手术治疗的踝关节骨折患者术后LOS的因素。
回顾性确定2004年1月1日至2010年12月31日期间622例踝关节骨折患者。查阅病历以获取性别、手术时间长度、固定方法、美国麻醉医师协会(ASA)身体状况评分、内科合并症和术后LOS。建立单变量和多变量模型以确定患者LOS的预测因素。从财务部门获取平均24小时住院的财务数据。
纳入622例患者。在线性回归分析中,ASA状态与LOS之间存在统计学显著关系(P < 0.001)。多元回归分析进一步描述了ASA与LOS之间的关系:ASA分类每增加1个单位,LOS平均增加3.42天(P < 0.001)。基于平均每天住院费用4503美元,ASA状态每增加1个单位导致费用增加15490美元。
我们的研究表明,ASA状态是接受踝关节骨折手术固定患者LOS的有力预测因素。对这些因素更全面的了解将导致更好的风险调整模型,用于衡量结果、确定公平报销以及潜在提高患者护理效率。
III级回顾性比较研究,将住院时间与包括ASA身体状况在内的许多变量进行回归分析。