Chevallier Marie, Ego Anne, Cans Christine, Debillon Thierry
Neonatology and Pediatric Intensive Care Unit, Grenoble University Hospital, Grenoble, France.
Clinical Research Center (CICO3), Grenoble University Hospital, Grenoble, France.
PLoS One. 2013 Dec 31;8(12):e83742. doi: 10.1371/journal.pone.0083742. eCollection 2013.
The objective of this study was to describe the French practice of hypothermia treatment (HT) in full-term newborns with hypoxic-ischemic encephalopathy (HIE) and to analyze the deviations from the guidelines of the French Society of Neonatology.
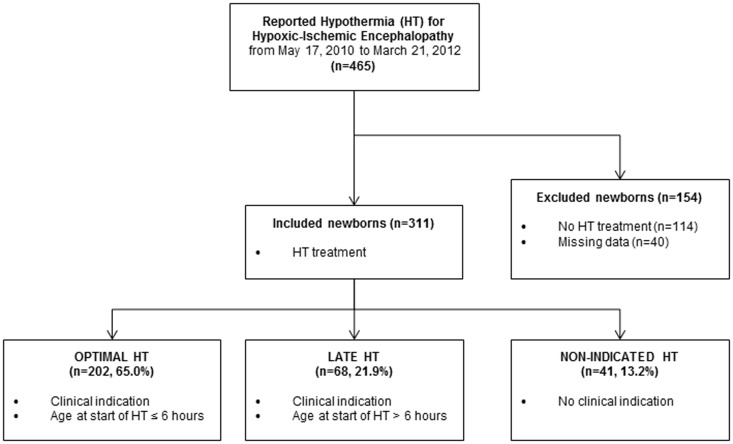
From May 2010 to March 2012 we recorded all cases of HIE treated by HT in a French national database. The population was divided into three groups, "optimal HT" (OHT), "late HT" (LHT) and "non-indicated" HT (NIHT), according to the guidelines.
Of the 311 newborns registered in the database and having HT, 65% were classified in the OHT group, 22% and 13% in the LHT and NIHT groups respectively. The severity of asphyxia and HIE were comparable between newborns with OHT and LHT, apart from EEG. HT was initiated at a mean time of 12 hours of life in the LHT group. An acute obstetrical event was more likely to be identified among newborns with LHT (46%), compared to OHT (34%) and NIHT (22%). There was a gradation in the rate of complications from the NIHT group (29%) to the LHT (38%) group and the OHT group (52%). Despite an insignificant difference in the rates of death or abnormal neurological examination at discharge, nearly 60% of newborns in the OHT group had an MRI showing abnormalities, compared to 44% and 49% in the LHT and NIHT groups respectively.
The conduct of the HT for HIE newborns is not consistent with French guidelines for 35% of newborns, 22% being explained by an excessive delay in the start of HT, 13% by the lack of adherence to the clinical indications. This first report illustrates the difficulties in implementing guidelines for HT and should argue for an optimization of perinatal care for HIE.
本研究的目的是描述法国对患有缺氧缺血性脑病(HIE)的足月儿进行低温治疗(HT)的实际情况,并分析与法国新生儿学会指南的偏差。
2010年5月至2012年3月,我们在一个法国国家数据库中记录了所有接受HT治疗的HIE病例。根据指南,将研究对象分为三组:“最佳HT”(OHT)组、“延迟HT”(LHT)组和“非适应证”HT(NIHT)组。
在数据库中登记并接受HT治疗的311例新生儿中,65%被归类为OHT组,22%和13%分别在LHT组和NIHT组。除脑电图外,OHT组和LHT组新生儿的窒息和HIE严重程度相当。LHT组HT开始的平均时间为生后12小时。与OHT组(34%)和NIHT组(22%)相比,LHT组新生儿中更有可能识别出急性产科事件(46%)。并发症发生率从NIHT组(29%)到LHT组(38%)再到OHT组(52%)呈逐渐升高趋势。尽管出院时死亡或神经系统检查异常的发生率差异无统计学意义,但OHT组近60%的新生儿MRI显示异常,而LHT组和NIHT组分别为44%和49%。
对于35%的HIE新生儿,HT的实施不符合法国指南,其中22%是由于HT开始时间过度延迟,13%是由于未遵循临床适应证。这篇首次报告说明了实施HT指南的困难,并应主张优化HIE围产期护理。