Ward Stephen Thomas, Mohammed Mohammed A, Walt Robert, Valori Roland, Ismail Tariq, Dunckley Paul
Centre for Liver Research and NIHR Birmingham Biomedical Research Unit, Level 5 Institute for Biomedical Research, University of Birmingham, Birmingham, UK.
School of Health Studies, University of Bradford, Bradford, UK.
Gut. 2014 Nov;63(11):1746-54. doi: 10.1136/gutjnl-2013-305973. Epub 2014 Jan 27.
The number of colonoscopies required to reach competency is not well established. The primary aim of this study was to determine the number of colonoscopies trainees need to perform to attain competency, defined by a caecal intubation rate (CIR) ≥90%. As competency depends on completion, we also investigated trainee factors that were associated with colonoscopy completion.
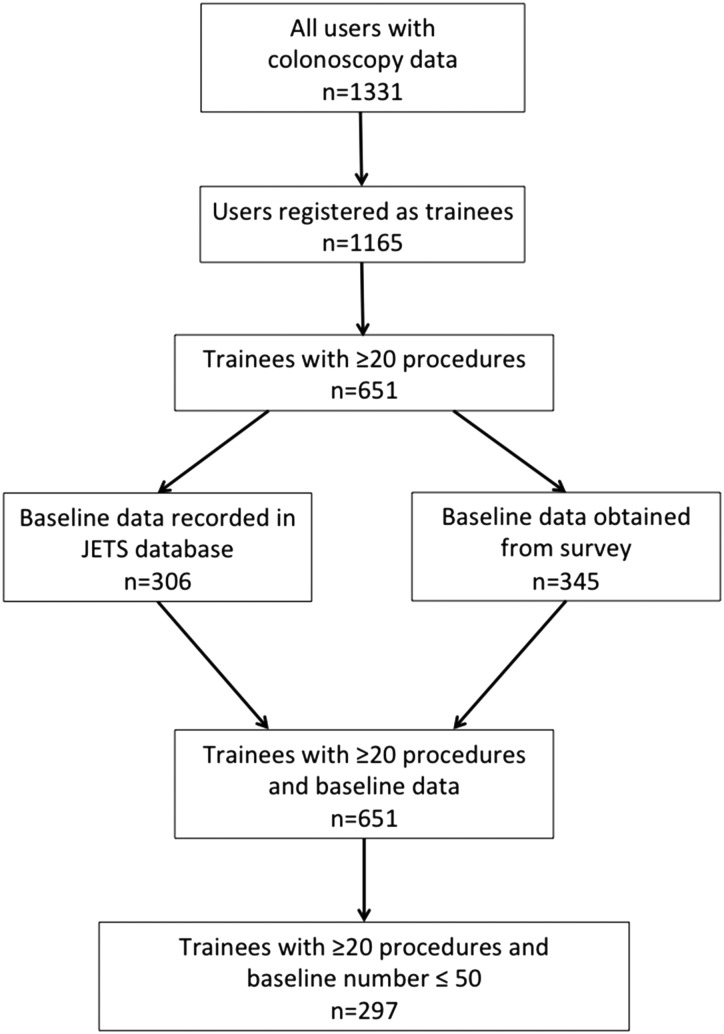
The Joint Advisory Group on GI Endoscopy in the UK has developed a trainee e-portfolio from which colonoscopy data were retrieved. Inclusion criteria were all trainees who had performed a total of ≥20 colonoscopies and had performed ≤50 colonoscopies prior to submission of data to the e-portfolio. The primary outcome measure was colonoscopy completion. The number of colonoscopies required to achieve CIR ≥90% was calculated by the moving average method and learning curve cumulative summation (LC-Cusum) analysis. To determine factors which determine colonoscopy completion, a mixed effect logistic regression model was developed which allowed for nesting of patients within trainees and nesting of patients within hospitals, with various patient, trainee and training factors entered as fixed effects.
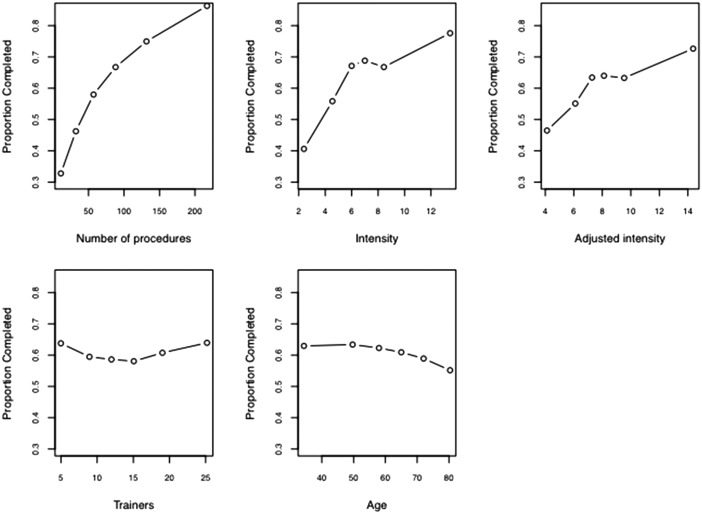
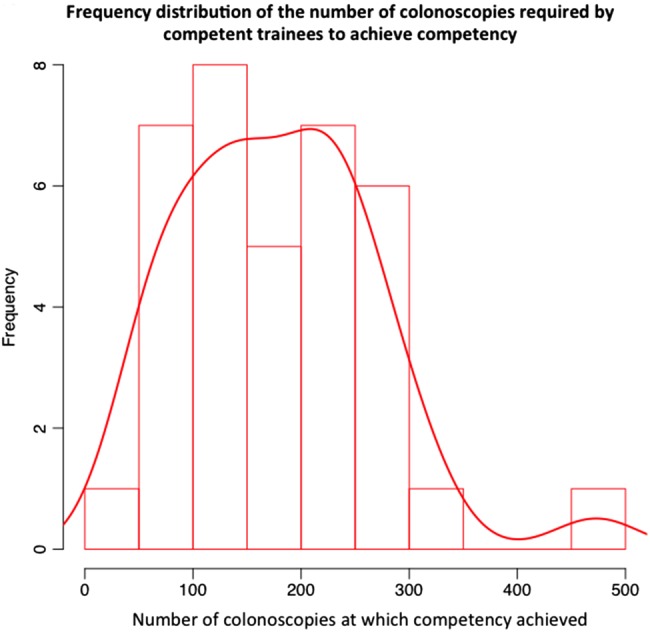
297 trainees undertook 36 730 colonoscopies. By moving average analysis, the cohort of trainees reached a CIR of 90% at 233 procedures. By LC-Cusum analysis, 41% of trainees were competent after 200 procedures. Of the trainee factors, the number of colonoscopies, intensity of training and previous flexible sigmoidoscopy experience were significant factors associated with colonoscopy completion.
This is the largest study to date investigating the number of procedures required to achieve competency in colonoscopy. The current training certification benchmark in the UK of 200 procedures does not appear to be an inappropriate minimum requirement. The LC-Cusum chart provides real time feedback on individual learning curves for trainees. The association of training intensity and flexible sigmoidoscopy experience with colonoscopy completion could be exploited in training programmes.
达到结肠镜检查能力所需的结肠镜检查次数尚未明确确定。本研究的主要目的是确定实习生达到能力(定义为盲肠插管率(CIR)≥90%)所需进行的结肠镜检查次数。由于能力取决于完成情况,我们还调查了与结肠镜检查完成相关的实习生因素。
英国胃肠内镜联合咨询小组开发了一个实习生电子档案袋,从中检索结肠镜检查数据。纳入标准为在向电子档案袋提交数据之前总共进行了≥20次结肠镜检查且≤50次结肠镜检查的所有实习生。主要结局指标是结肠镜检查完成情况。通过移动平均法和学习曲线累积求和(LC-Cusum)分析计算达到CIR≥90%所需的结肠镜检查次数。为了确定决定结肠镜检查完成情况的因素,开发了一个混合效应逻辑回归模型,该模型允许患者在实习生内嵌套以及患者在医院内嵌套,并将各种患者、实习生和培训因素作为固定效应输入。
297名实习生进行了36730次结肠镜检查。通过移动平均分析,实习生队列在233次操作时达到了90%的CIR。通过LC-Cusum分析,41%的实习生在200次操作后达到能力标准。在实习生因素中,结肠镜检查次数、培训强度和以前的乙状结肠镜检查经验是与结肠镜检查完成相关的重要因素。
这是迄今为止调查达到结肠镜检查能力所需操作次数的最大规模研究。英国目前200次操作的培训认证基准似乎并非不适当的最低要求。LC-Cusum图表为实习生提供了关于个人学习曲线的实时反馈。培训强度和乙状结肠镜检查经验与结肠镜检查完成情况之间的关联可在培训计划中加以利用。