Prinja Shankar, Jeet Gursimer, Verma Ramesh, Kumar Dinesh, Bahuguna Pankaj, Kaur Manmeet, Kumar Rajesh
School of Public Health, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
Department of Community Medicine, Pt. BD Sharma Post Graduate Institute of Medical Sciences, Rohtak, Haryana, India.
PLoS One. 2014 Mar 13;9(3):e91781. doi: 10.1371/journal.pone.0091781. eCollection 2014.
We assessed overall annual and unit cost of delivering package of services and specific services at sub-centre level by CHWs and cost effectiveness of Government of India's policy of introducing a second auxiliary nurse midwife (ANM) at the sub-centre compared to scenario of single ANM sub-centre.
We undertook an economic costing of health services delivered by CHWs, from a health system perspective. Bottom-up costing method was used to collect data on resources spent in 50 randomly selected sub-centres selected from 4 districts. Mean unit cost along with its 95% confidence intervals were estimated using bootstrap method. Multiple linear regression model was used to standardize cost and assess its determinants.
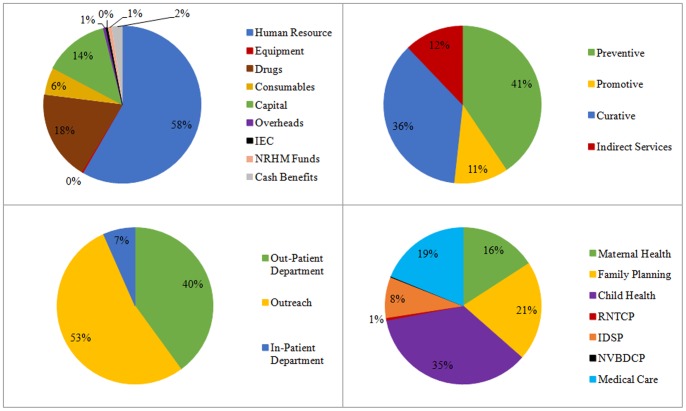
Annually it costs INR 1.03 million (USD 19,381), or INR 187 (USD 3.5) per capita per year, to provide a package of preventive, curative and promotive services through community health workers. Unit costs for antenatal care, postnatal care, DOTS treatment and immunization were INR 525 (USD 10) per full ANC care, INR 767 (USD 14) per PNC case registered, INR 974 (USD 18) per DOTS treatment completed and INR 97 (USD 1.8) per child immunized in routine immunization respectively. A 10% increase in human resource costs results in 6% rise in per capita cost. Similarly, 10% increment in the ANC case registered per provider through-put results in a decline in unit cost ranging from 2% in the event of current capacity utilization to 3% reduction in case of full capacity utilization. Incremental cost of introducing 2nd ANM at sub-centre level per unit percent increase ANC coverage was INR 23,058 (USD 432).
Our estimates would be useful in undertaking full economic evaluations or equity analysis of CHW programs. Government of India's policy of hiring 2nd ANM at sub-centre level is very cost effective from Indian health system perspective.
我们评估了社区卫生工作者在基层医疗中心提供一揽子服务和特定服务的年度总成本及单位成本,以及与单一辅助护士助产士(ANM)基层医疗中心的情况相比,印度政府在基层医疗中心引入第二名辅助护士助产士政策的成本效益。
我们从卫生系统角度对社区卫生工作者提供的卫生服务进行了经济成本核算。采用自下而上的成本核算方法,收集了从4个地区随机选取的50个基层医疗中心的资源支出数据。使用自助法估计平均单位成本及其95%置信区间。采用多元线性回归模型对成本进行标准化并评估其决定因素。
通过社区卫生工作者提供一揽子预防、治疗和促进性服务,每年花费103万印度卢比(19381美元),即人均每年187印度卢比(3.5美元)。产前护理、产后护理、直接观察短程化疗(DOTS)治疗和免疫接种的单位成本分别为每次完整的产前护理525印度卢比(10美元)、每次登记的产后护理病例767印度卢比(14美元)、每次完成的DOTS治疗974印度卢比(18美元)以及常规免疫接种中每名儿童97印度卢比(1.8美元)。人力资源成本增加10%会导致人均成本上升6%。同样,每个提供者处理的产前护理病例增加10%,单位成本会下降,当前产能利用率情况下下降2%,满负荷产能利用率情况下下降3%。在基层医疗中心引入第二名ANM,每单位百分比增加的产前护理覆盖率的增量成本为23058印度卢比(432美元)。
我们的估计结果将有助于对社区卫生工作者项目进行全面经济评估或公平性分析。从印度卫生系统角度来看,印度政府在基层医疗中心雇佣第二名ANM的政策具有很高的成本效益。