1 University of California, Los Angeles, CA. 2 XDx Inc., Brisbane, CA. 3 Stanford University Medical Center, Stanford, CA. 4 VA Palo Alto Health Care System, Palo Alto, CA. 5 University of Pittsburgh Medical Center, Pittsburgh, PA. 6 Intermountain Medical Center and Intermountain Healthcare, Salt Lake City, UT. 7 Cleveland Clinic, Cleveland, OH. 8 Hospital of the University of Pennsylvania, Philadelphia, PA. 9 Mid America Heart Institute, Saint Luke's Hospital, Kansas City, MO. 10 University of Chicago Medical Center, Chicago, IL. 11 Northwestern University, Chicago, IL. 12 Washington University School of Medicine, St. Louis, MO. 13 Newark Beth Israel Medical Center, Newark, NJ. 14 Texas Heart Institute, Houston, TX. 15 Columbia University, New York City, NY. 16 Address correspondence to: Mario Deng, M.D., F.A.C.C., F.E.S.C., Advanced Heart Failure/Mechanical Support/Heart Transplant, David Geffen School of Medicine at UCLA, Ronald Reagan UCLA Medical Center, 100 Medical Plaza Drive, Suite 630 Los Angeles, CA 90095.
Transplantation. 2014 Mar 27;97(6):708-14. doi: 10.1097/01.TP.0000443897.29951.cf.
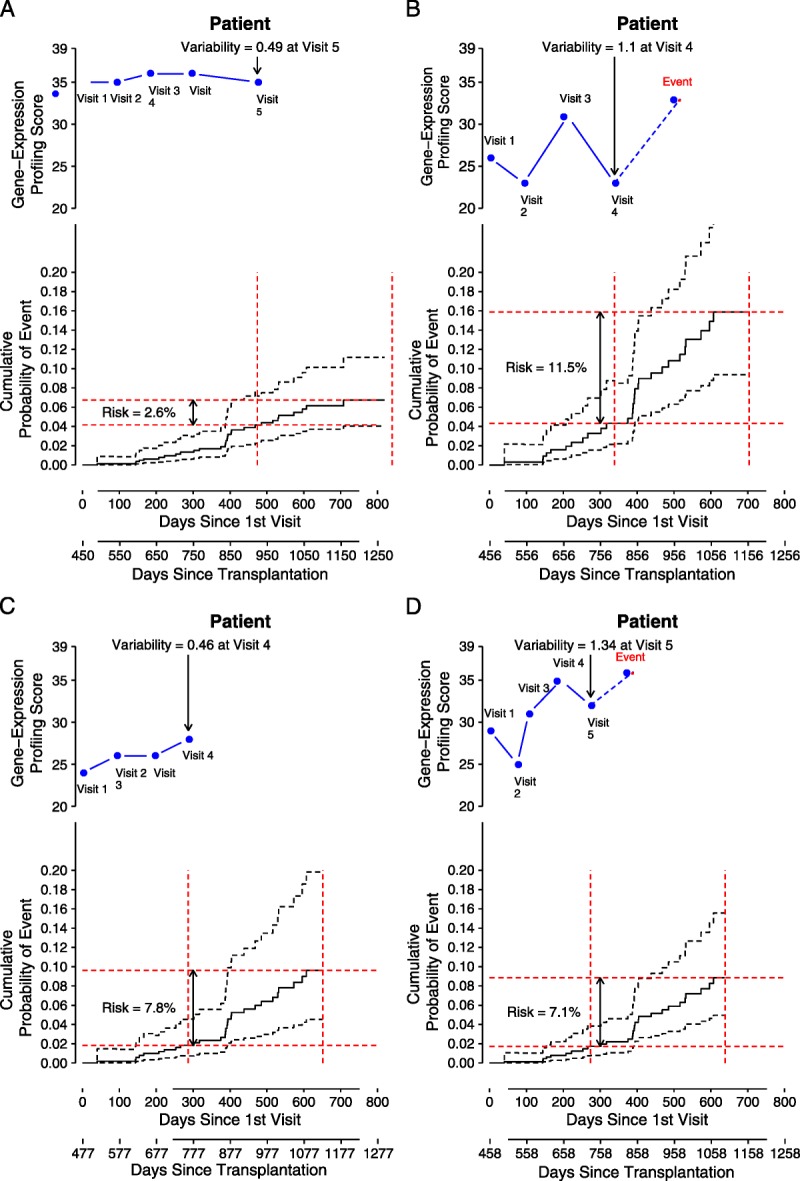
Gene expression profiling test scores have primarily been used to identify heart transplant recipients who have a low probability of rejection at the time of surveillance testing. We hypothesized that the variability of gene expression profiling test scores within a patient may predict risk of future events of allograft dysfunction or death.
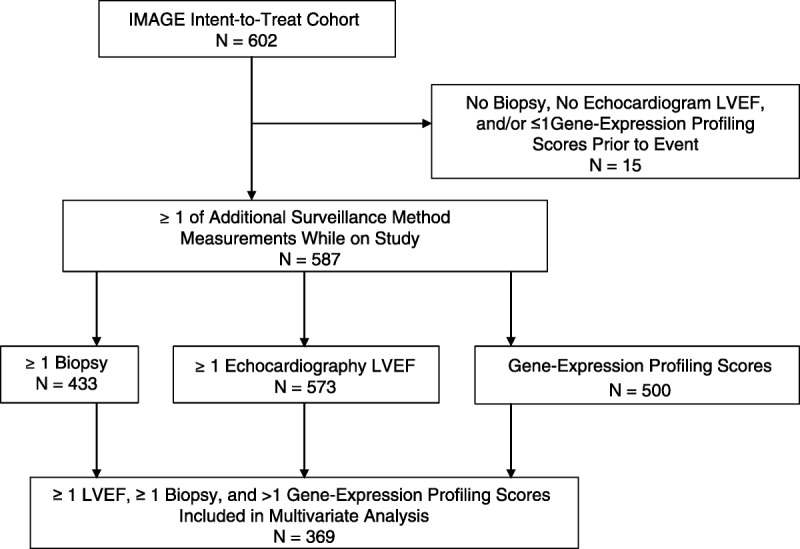
Patients from the IMAGE study with rejection surveillance gene expression profiling tests performed at 1- to 6-month intervals were selected for this cohort study. Gene expression profiling score variability was defined as the standard deviation of an individual's cumulative test scores. Gene expression profiling ordinal score (range, 0-39), threshold score (binary value=1 if ordinal score ≥ 34), and score variability were studied in multivariate Cox regression models to predict future clinical events.
Race, age at time of transplantation, and time posttransplantation were significantly associated with future events in the univariate analysis. In the multivariate analyses, gene expression profiling score variability, but not ordinal scores or scores over threshold, was independently associated with future clinical events. The regression coefficient P values were <0.001, 0.46, and 0.773, for gene expression profiling variability, ordinal, and threshold scores, respectively. The hazard ratio for a 1 unit increase in variability was 1.76 (95% CI, 1.4-2.3).
The variability of a heart recipient's gene expression profiling test scores over time may provide prognostic utility. This information is independent of the probability of acute cellular rejection at the time of testing that is rendered from a single ordinal gene-expression profiling test score.
基因表达谱测试评分主要用于识别在监测测试时排斥反应可能性较低的心脏移植受者。我们假设患者体内基因表达谱测试评分的变异性可能预测同种异体移植物功能障碍或死亡的未来事件风险。
从 IMAGE 研究中选择在 1-6 个月间隔进行排斥监测基因表达谱测试的患者进行这项队列研究。基因表达谱评分变异性定义为个体累积测试评分的标准差。基因表达谱有序评分(范围 0-39)、阈值评分(有序评分≥34 时为二进制值=1)和评分变异性在多变量 Cox 回归模型中用于预测未来临床事件。
在单变量分析中,种族、移植时的年龄和移植后时间与未来事件显著相关。在多变量分析中,基因表达谱评分变异性,而不是有序评分或超过阈值的评分,与未来临床事件独立相关。基因表达谱变异性、有序和阈值评分的回归系数 P 值分别为<0.001、0.46 和 0.773。变异性增加 1 个单位的风险比为 1.76(95%CI,1.4-2.3)。
心脏受者基因表达谱测试评分随时间的变异性可能提供预后效用。该信息独立于测试时基于单次有序基因表达谱测试评分得出的急性细胞排斥的可能性。