Weldearegawi Berhe, Spigt Mark, Berhane Yemane, Dinant Geertjan
Department of Public Health, College of Health Sciences, Mekelle University, Mekelle, Ethiopia; CAPHRI, School for Public Health and Primary Care, Maastricht University, Maastricht, Netherlands.
Addis Continental Institute of Public Health, Addis Ababa, Ethiopia.
PLoS One. 2014 Mar 27;9(3):e93099. doi: 10.1371/journal.pone.0093099. eCollection 2014.
Over the last fifty years the world has seen enormous decline in mortality rates. However, in low-income countries, where vital registration systems are absent, mortality statistics are not easily available. The recent economic growth of Ethiopia and the parallel large scale healthcare investments make investigating mortality figures worthwhile.
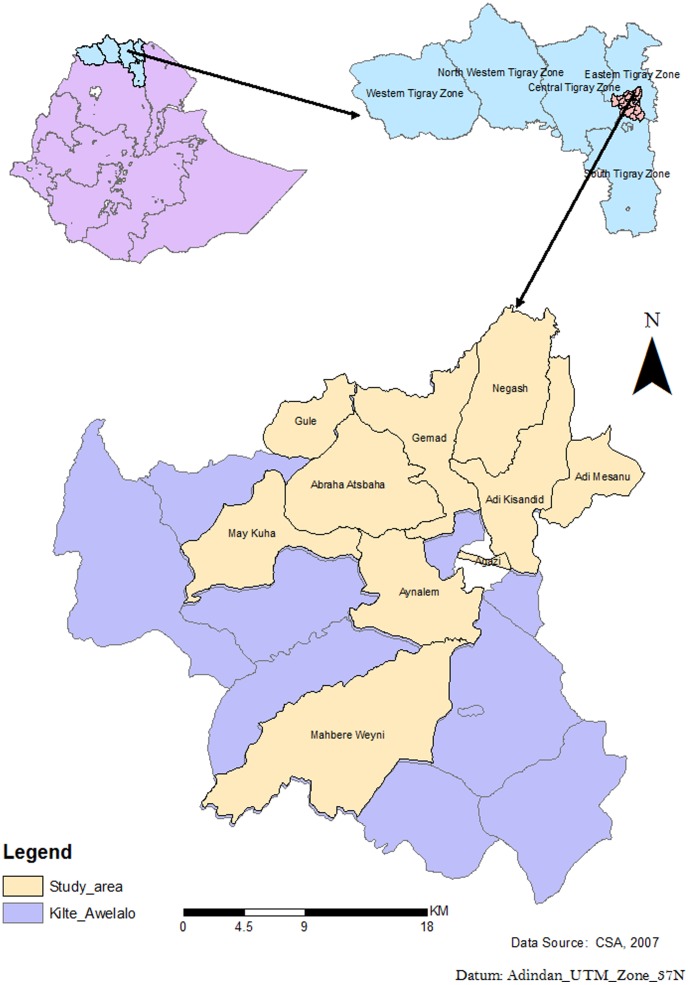
Longitudinal health and demographic surveillance data collected from September 11, 2009 to September 10, 2012 were analysed. We computed incidence of mortality, overall and stratified by background variables. Poisson regression was used to test for a linear trend in the standardized mortality rates. Cox-regression analysis was used to identify predictors of mortality. Households located at <2300 meter and ≥ 2300 meter altitude were defined to be midland and highland, respectively.
An open cohort, with a baseline population of 66,438 individuals, was followed for three years to generate 194,083 person-years of observation. The crude mortality rate was 4.04 (95% CI: 3.77, 4.34) per 1,000 person-years. During the follow-up period, incidence of mortality significantly declined among under five (P<0.001) and 5-14 years old (P<0.001), whereas it increased among 65 years and above (P<0.001). Adjusted for other covariates, mortality was higher in males (hazard ratio (HR) = 1.42, 95% CI: 1.22, 1.66), rural population (HR = 1.74, 95% CI: 1.32, 2.31), highland (HR = 1.20, 95% CI: 1.03, 1.40) and among those widowed (HR = 2.25, 95% CI: 1.81, 2.80) and divorced (HR = 1.80, 95% CI: 1.30, 2.48).
Overall mortality rate was low. The level and patterns of mortality indicate changes in the epidemiology of major causes of death. Certain population groups had significantly higher mortality rates and further research is warranted to identify causes of higher mortality in those groups.
在过去五十年间,全球死亡率大幅下降。然而,在缺乏人口动态登记系统的低收入国家,死亡率统计数据难以获取。埃塞俄比亚近期的经济增长以及同时进行的大规模医疗投资使得对死亡率数据的调查变得很有价值。
对2009年9月11日至2012年9月10日收集的纵向健康和人口监测数据进行分析。我们计算了总体死亡率以及按背景变量分层的死亡率。采用泊松回归检验标准化死亡率的线性趋势。使用Cox回归分析确定死亡率的预测因素。海拔低于2300米和海拔≥2300米的家庭分别被定义为中部地区和高地地区。
一个开放队列,基线人口为66438人,随访三年,产生了194083人年的观察数据。粗死亡率为每1000人年4.04(95%置信区间:3.77,4.34)。在随访期间,五岁以下儿童(P<0.001)和5 - 14岁儿童(P<0.001)的死亡率显著下降,而65岁及以上人群的死亡率则有所上升(P<0.001)。在对其他协变量进行调整后,男性(风险比(HR)= 1.42,95%置信区间:1.22,1.66)、农村人口(HR = 1.74,95%置信区间:1.32,2.31)、高地地区人口(HR = 1.20,95%置信区间:1.03,1.40)以及丧偶者(HR = 2.25,95%置信区间:1.81,2.80)和离婚者(HR = 1.80,95%置信区间:1.30,2.48)的死亡率更高。
总体死亡率较低。死亡率的水平和模式表明主要死因的流行病学发生了变化。某些人群的死亡率显著较高,有必要进一步研究以确定这些人群中高死亡率的原因。