Carduff Emma, Finucane Anne, Kendall Marilyn, Jarvis Alison, Harrison Nadine, Greenacre Jane, Murray Scott A
Primary Palliative Care Research Group, Centre for Population Health Sciences, The University of Edinburgh, Medical School, Teviot Place, Edinburgh, UK.
BMC Fam Pract. 2014 Apr 2;15:48. doi: 10.1186/1471-2296-15-48.
Approximately 10% of the UK population have an unpaid caring role for a family member or friend. Many of these carers make a significant contribution to supporting patients at the end of life. Carers can experience poor physical and psychosocial wellbeing, yet they remain largely unsupported by health and social care services. Despite initiatives for general practices to identify carers and their needs, many remain unidentified. Neither are carers self-identifying and requesting support. This study set out to explore the barriers to, and consider strategies for, identifying carers in primary care.
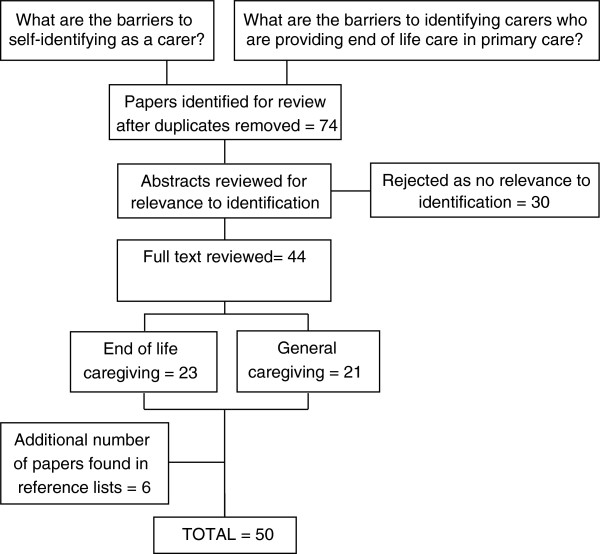
We integrated findings from three data sources - a review of the caregiving literature; a workshop with researchers who have undertaken research with those caring at the end of life, and focus groups with carers and health professionals.
Three categories of barrier emerged. 1) Taking on the care of another person is often a gradual process, carers did not immediately identify with being a 'carer' - preferring to think of themselves in relational terms to the patient e.g. spouse, sibling, son or daughter. Often it was health and social care professionals who encouraged carers to consider themselves as an unpaid carer. 2) As the cared-for person's condition deteriorated, the caring role often became all-encompassing so that carers were managing competing demands, and felt unable to look after their own needs as well as those of the cared-for person. 3) There was ambiguity about the legitimacy of carer needs and about the role of the primary health care team in supporting carers, from both the perspective of the carers and the health professionals. GPs were thought to be reactive rather than proactive which discouraged carers from asking for help.
The needs of carers have to be legitimised to ensure primary care staff are proactive in their approach and carers are empowered to utilise the support available. Strategies to identify carers have to be sensitive to the complex dynamics of a caring relationship as well as the primary care context. Identification is a key factor in improving support for carers themselves and to enable them to support the patient.
在英国,约10%的人口承担着照顾家庭成员或朋友的非带薪护理工作。这些护理者中有许多人在临终关怀患者方面做出了重大贡献。护理者的身心健康状况可能较差,但他们在很大程度上仍未得到卫生和社会护理服务的支持。尽管有倡议要求全科医疗服务机构识别护理者及其需求,但仍有许多护理者未被识别出来。护理者也不会主动表明身份并寻求支持。本研究旨在探讨在初级医疗保健中识别护理者的障碍,并考虑相关策略。
我们整合了三个数据源的研究结果——对护理文献的综述;与对临终关怀护理者进行研究的研究人员举办的研讨会;以及与护理者和健康专业人员进行的焦点小组讨论。
出现了三类障碍。1)承担照顾他人的责任通常是一个渐进的过程,护理者不会立即认同自己是“护理者”——他们更倾向于从与患者的关系角度来思考自己,如配偶、兄弟姐妹、儿子或女儿。通常是卫生和社会护理专业人员鼓励护理者将自己视为非带薪护理者。2)随着被照顾者病情恶化,护理角色往往变得无所不包,以至于护理者要应对相互冲突的需求,感到无法兼顾自己和被照顾者的需求。3)从护理者和健康专业人员的角度来看,护理者需求的合理性以及初级医疗保健团队在支持护理者方面的作用都不明确。全科医生被认为是被动应对而非主动出击,这使得护理者不愿寻求帮助。
必须使护理者的需求合法化,以确保初级医疗保健人员积极主动地采取措施,使护理者有能力利用现有的支持。识别护理者的策略必须考虑到护理关系的复杂动态以及初级医疗保健环境。识别是改善对护理者自身的支持并使其能够支持患者的关键因素。