Neonatal and Paediatric Intensive Care Unit, Children's Hospital Lucerne, Spitalstrasse, Lucerne 16 CH-6000, Switzerland.
BMC Med Educ. 2014 Apr 3;14:69. doi: 10.1186/1472-6920-14-69.
As a conceptual review, this paper will debate relevant learning theories to inform the development, design and delivery of an effective educational programme for simulated team training relevant to health professionals.
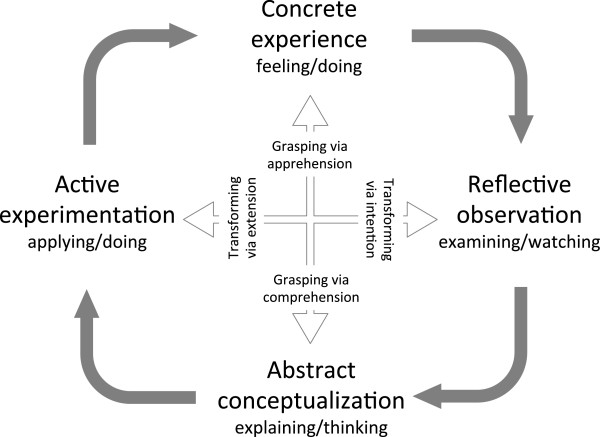
Kolb's experiential learning theory is used as the main conceptual framework to define the sequence of activities. Dewey's theory of reflective thought and action, Jarvis modification of Kolb's learning cycle and Schön's reflection-on-action serve as a model to design scenarios for optimal concrete experience and debriefing for challenging participants' beliefs and habits. Bandura's theory of self-efficacy and newer socio-cultural learning models outline that for efficient team training, it is mandatory to introduce the social-cultural context of a team.
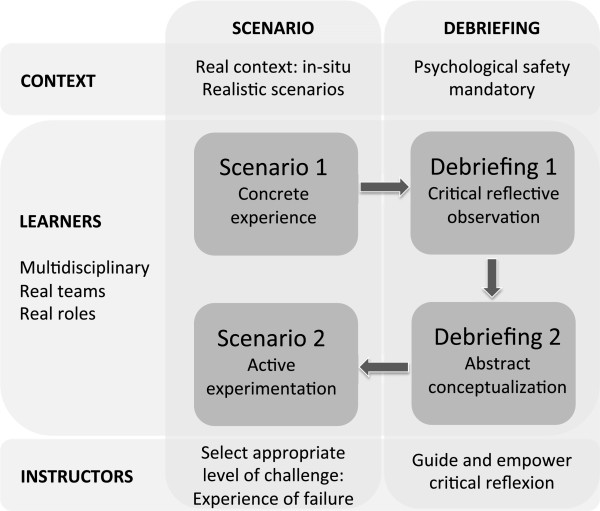
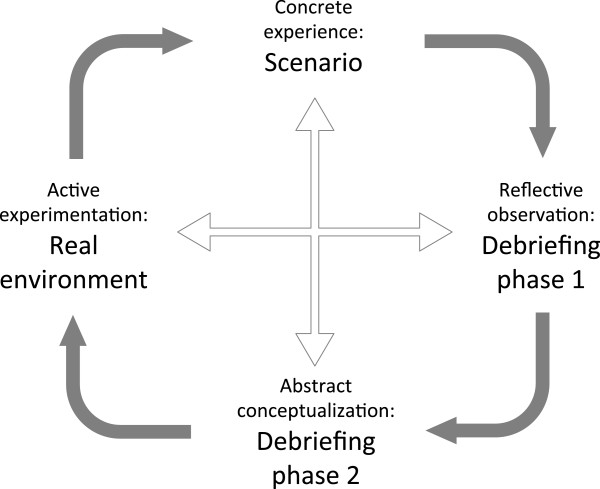
The ideal simulated team training programme needs a scenario for concrete experience, followed by a debriefing with a critical reflexive observation and abstract conceptualisation phase, and ending with a second scenario for active experimentation. Let them re-experiment to optimise the effect of a simulated training session. Challenge them to the edge: The scenario needs to challenge participants to generate failures and feelings of inadequacy to drive and motivate team members to critical reflect and learn. Not experience itself but the inadequacy and contradictions of habitual experience serve as basis for reflection. Facilitate critical reflection: Facilitators and group members must guide and motivate individual participants through the debriefing session, inciting and empowering learners to challenge their own beliefs and habits. To do this, learners need to feel psychological safe. Let the group talk and critical explore. Motivate with reality and context: Training with multidisciplinary team members, with different levels of expertise, acting in their usual environment (in-situ simulation) on physiological variables is mandatory to introduce cultural context and social conditions to the learning experience. Embedding in situ team training sessions into a teaching programme to enable repeated training and to assess regularly team performance is mandatory for a cultural change of sustained improvement of team performance and patient safety.
作为概念性综述,本文将讨论相关学习理论,为健康专业人员模拟团队培训的有效教育计划的开发、设计和实施提供信息。
科尔布的体验式学习理论被用作主要的概念框架,以定义活动序列。杜威的反思性思维和行动理论、贾维斯对科尔布学习周期的修改以及舍恩的行动反思为设计最佳具体体验场景和为具有挑战性的参与者的信念和习惯提供反馈提供了模型。班杜拉的自我效能理论和更新的社会文化学习模型指出,为了进行有效的团队培训,必须引入团队的社会文化背景。
理想的模拟团队培训计划需要一个具体体验的场景,随后是一个具有批判性反思观察和抽象概念化阶段的反馈,最后是第二个主动实验的场景。让他们重新进行实验,以优化模拟培训课程的效果。挑战他们的极限:场景需要挑战参与者,让他们产生失败感和不足感,从而激励和激发团队成员进行批判性反思和学习。不是体验本身,而是习惯性体验的不足和矛盾为反思提供了基础。促进批判性反思:促进者和小组成员必须在反馈会议上指导和激励个别参与者,激励和授权学习者挑战自己的信念和习惯。要做到这一点,学习者需要感到心理安全。让小组进行讨论和批判性探索。用现实和情境来激励:培训需要有不同专业水平的多学科团队成员,在他们通常的环境(现场模拟)中进行生理变量的操作,这是将文化背景和社会条件引入学习体验的必要条件。将现场团队培训课程嵌入教学计划中,以便进行重复培训并定期评估团队绩效,对于团队绩效和患者安全的持续改进的文化变革是必要的。