Hanson Kristin A, Agashivala Neetu, Wyrwich Kathleen W, Raimundo Karina, Kim Edward, Brandes David W
UBC: An Express Scripts Company, Dorval, QC, Canada.
Novartis Pharmaceuticals Corporation East Hanover, NJ, USA.
Patient Prefer Adherence. 2014 Apr 3;8:415-22. doi: 10.2147/PPA.S53140. eCollection 2014.
Multiple sclerosis (MS) is a complex disease with many therapeutic options. Little is known about how neurologists select particular disease-modifying therapies (DMTs) for their patients.
To understand how neurologists make decisions regarding the prescription of DMTs for patients with MS, and to explore neurologists' experiences with individual DMTs.
From December 2012 to January 2013, members of a nationwide physician market research panel were sent an online study invitation with a link to a survey website. Eligible neurologists were included if they currently practice medicine in the United States, and if they treat ≥20 patients with MS.
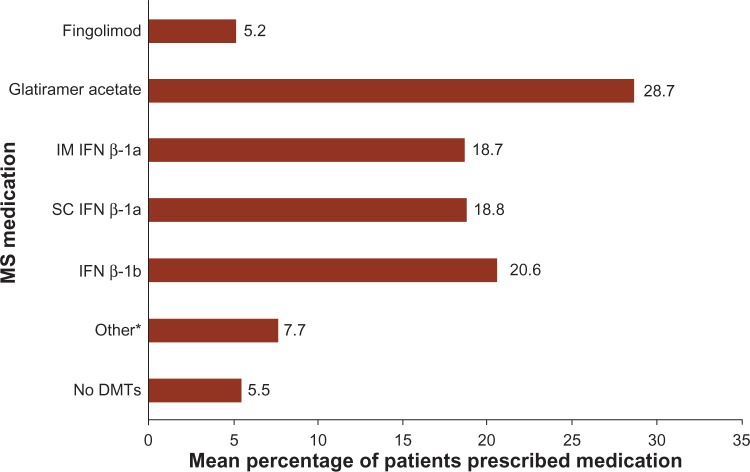
A total of 102 neurologists (n=63 general neurologists; n=39 MS specialists; 81.4% male) completed the survey. The mean (standard deviation) number of years in practice since completing medical training was 16.4 (8.6) years. Overall, the most commonly prescribed DMTs were subcutaneous interferon (IFN) β-1a and glatiramer acetate; approximately 5.5% of patients were untreated. The most important attributes of DMT medication selection were (in order of importance) efficacy, safety, tolerability, patient preference, and convenience. The DMT with the highest neurologist-reported percentage of patients who were "Very/Extremely Satisfied" with their therapy was fingolimod (31.0%), followed by glatiramer acetate (13.9%; P=0.017). Compared with fingolimod (94.0%), significantly fewer (P<0.05) neurologists reported that "All/Most" of their patients were adherent to treatment with glatiramer acetate (78.0%), subcutaneous IFN β-1a (84.0%), and IFN β-1b (75.0%); no significant differences were observed with intramuscular IFN β-1a (92.9%; P=0.75). Patients' calls to neurologists' offices were most commonly related to side effects for all self-injectable DMTs, whereas calls about fingolimod primarily involved insurance coverage issues.
Our survey results showed that very few patients with MS did not received any DMT. Among the DMTs available at the time of the survey, neurologists reported that patients were most satisfied with, and adherent to, fingolimod, but these patients also faced more problems with insurance coverage when compared with those taking self-injectable DMTs.
多发性硬化症(MS)是一种有多种治疗选择的复杂疾病。关于神经科医生如何为患者选择特定的疾病修正疗法(DMTs),人们知之甚少。
了解神经科医生如何就MS患者的DMT处方做出决策,并探讨神经科医生使用个别DMT的经验。
2012年12月至2013年1月,向全国范围内的医生市场研究小组成员发送了带有调查网站链接的在线研究邀请。符合条件的神经科医生包括目前在美国行医且治疗≥20例MS患者的医生。
共有102名神经科医生(n = 63名普通神经科医生;n = 39名MS专科医生;81.4%为男性)完成了调查。自完成医学培训以来的平均(标准差)执业年限为16.4(8.6)年。总体而言,最常处方的DMT是皮下注射干扰素(IFN)β-1a和醋酸格拉替雷;约5.5%的患者未接受治疗。DMT药物选择的最重要属性(按重要性排序)是疗效、安全性、耐受性、患者偏好和便利性。神经科医生报告的患者对其治疗“非常/极其满意”比例最高的DMT是芬戈莫德(31.0%),其次是醋酸格拉替雷(13.9%;P = 0.017)。与芬戈莫德(94.0%)相比,报告其“所有/大多数”患者坚持使用醋酸格拉替雷(78.0%)、皮下注射IFNβ-1a(84.0%)和IFNβ-1b(75.0%)治疗的神经科医生明显较少(P<0.05);肌肉注射IFNβ-1a(92.9%;P = 0.75)未观察到显著差异。患者致电神经科医生办公室最常见的原因是所有自我注射DMT的副作用,而关于芬戈莫德的致电主要涉及保险覆盖问题。
我们的调查结果显示,极少有MS患者未接受任何DMT治疗。在调查时可用的DMT中,神经科医生报告患者对芬戈莫德最满意且依从性最高,但与使用自我注射DMT的患者相比,这些患者在保险覆盖方面也面临更多问题。