Saint Luke's Mid America Heart Institute, Kansas City, MO, USA University of Missouri-Kansas City, Kansas City, MO, USA
Saint Luke's Mid America Heart Institute, Kansas City, MO, USA University of Missouri-Kansas City, Kansas City, MO, USA.
Eur J Prev Cardiol. 2015 Jun;22(6):779-87. doi: 10.1177/2047487314533622. Epub 2014 Apr 16.
While patients with diabetes mellitus (DM) have more extensive coronary disease and worse survival after acute myocardial infarction (AMI) than patients without DM, data on whether they experience more angina are conflicting.
We examined angina prevalence over the year following AMI among 3367 patients, including 1080 (32%) with DM, from 24 US hospitals enrolled in the TRIUMPH registry from 2005 to 2008.
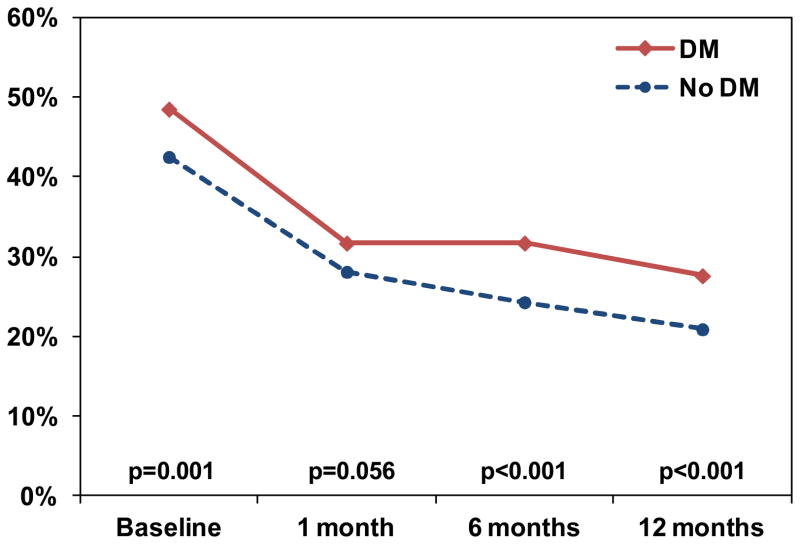
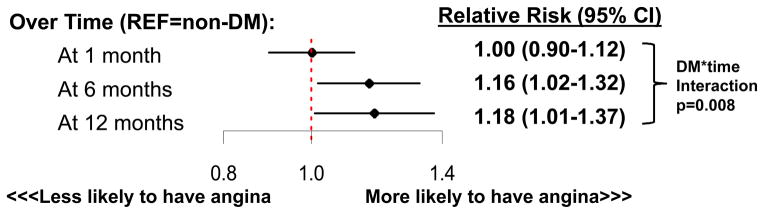
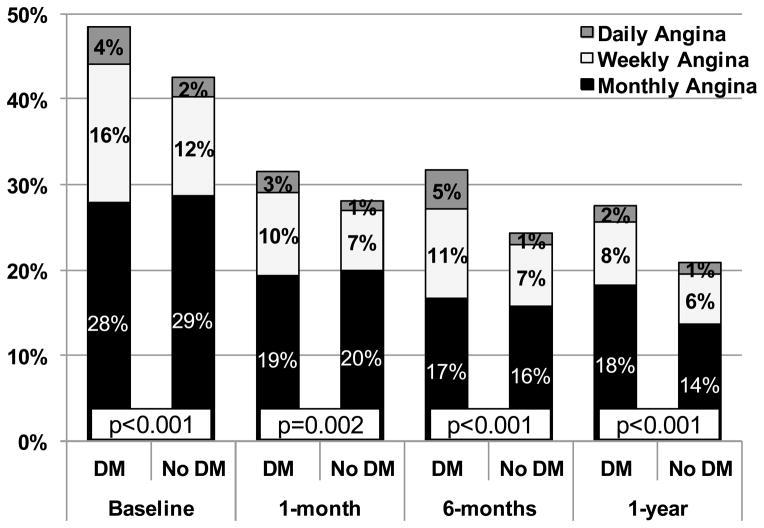
Patients with vs. without DM were more likely to be treated with antianginal medications both at discharge and over follow up. Despite more aggressive angina therapy, patients with vs. without DM had higher prevalence and severity of angina prior to AMI (49 vs. 43%, p = 0.001) and at each follow-up assessment, although rates of angina declined in both groups over time. In a hierarchical, multivariable, repeated-measures model that adjusted for multiple demographic and clinical factors including severity of coronary disease and in-hospital revascularization, DM was associated with a greater odds of angina over the 12 months of follow up; this association increased in magnitude over time (12-month OR 1.18, 95% CI 1.01-1.37; DM*time pinteraction = 0.008).
Contrary to conventional wisdom, angina is more prevalent and more severe among patients with DM, both prior to and following AMI. This effect is amplified over time and independent of patient and treatment factors, including the presence of multivessel disease and coronary revascularization. This increased burden of angina may be due to more diffuse nature of coronary disease, more rapid progression of coronary disease over time, or greater myocardial demand among DM patients.
患有糖尿病(DM)的患者在发生急性心肌梗死(AMI)后,其冠状动脉疾病比非糖尿病患者更为广泛,且生存率更差,但关于其是否经历更多心绞痛的证据存在冲突。
我们研究了 2005 年至 2008 年间,来自美国 24 家医院的 TRIUMPH 注册研究中,3367 例 AMI 患者(包括 1080 例(32%)DM 患者)在 AMI 后一年内的心绞痛发生率。
与无 DM 患者相比,DM 患者在出院时和随访期间更有可能接受抗心绞痛药物治疗。尽管进行了更积极的抗心绞痛治疗,但 DM 患者在 AMI 之前和每次随访评估时,其心绞痛的发生率和严重程度均较高(49%比 43%,p=0.001),尽管两组的心绞痛发生率随时间推移均呈下降趋势。在一个分层、多变量、重复测量模型中,该模型调整了多个人口统计学和临床因素,包括冠状动脉疾病严重程度和院内血运重建,DM 与随访 12 个月内的心绞痛发生几率较高相关;随着时间的推移,这种相关性的程度增大(12 个月的 OR 1.18,95%CI 1.01-1.37;DM*时间交互作用 p 值=0.008)。
与传统观点相反,DM 患者在发生 AMI 之前和之后,其心绞痛的发生率和严重程度均更高。这种影响随时间而放大,且独立于患者和治疗因素,包括多血管疾病和冠状动脉血运重建的存在。DM 患者心绞痛负担增加的原因可能是由于冠状动脉疾病的弥漫性更强,随着时间的推移冠状动脉疾病进展更快,或心肌需求更大。