Department of Intensive Care Medicine, Academic Medical Center, University of Amsterdam, Meibergdreef 9, G3-228, 1105 AZ Amsterdam, The Netherlands.
BMC Pulm Med. 2014 Apr 26;14:72. doi: 10.1186/1471-2466-14-72.
The acute respiratory distress syndrome (ARDS) is a common, devastating complication of critical illness that is characterized by pulmonary injury and inflammation. The clinical diagnosis may be improved by means of objective biological markers. Electronic nose (eNose) technology can rapidly and non-invasively provide breath prints, which are profiles of volatile metabolites in the exhaled breath. We hypothesized that breath prints could facilitate accurate diagnosis of ARDS in intubated and ventilated intensive care unit (ICU) patients.
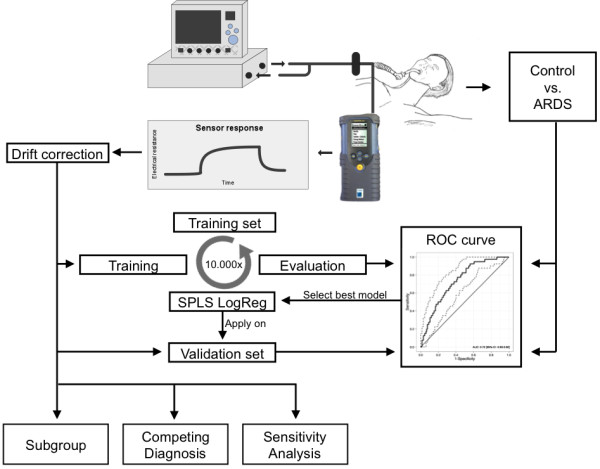
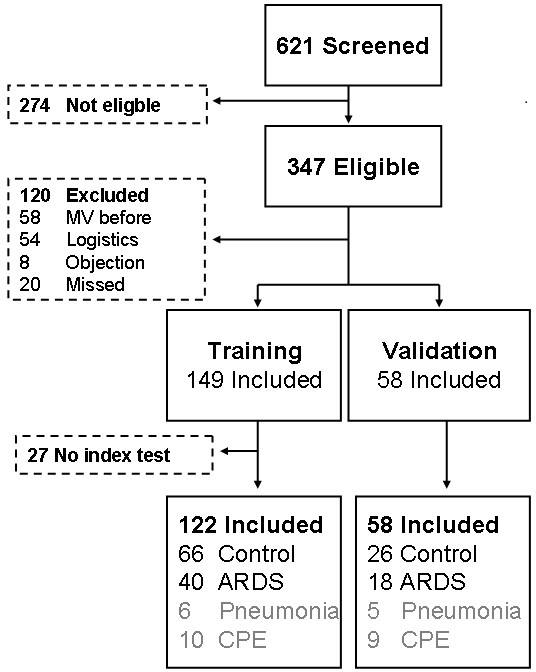
Prospective single-center cohort study with training and temporal external validation cohort. Breath of newly intubated and mechanically ventilated ICU-patients was analyzed using an electronic nose within 24 hours after admission. ARDS was diagnosed and classified by the Berlin clinical consensus definition. The eNose was trained to recognize ARDS in a training cohort and the diagnostic performance was evaluated in a temporal external validation cohort.
In the training cohort (40 patients with ARDS versus 66 controls) the diagnostic model for ARDS showed a moderate discrimination, with an area under the receiver-operator characteristic curve (AUC-ROC) of 0.72 (95%-confidence interval (CI): 0.63-0.82). In the external validation cohort (18 patients with ARDS versus 26 controls) the AUC-ROC was 0.71 [95%-CI: 0.54 - 0.87]. Restricting discrimination to patients with moderate or severe ARDS versus controls resulted in an AUC-ROC of 0.80 [95%-CI: 0.70 - 0.90]. The exhaled breath profile from patients with cardiopulmonary edema and pneumonia was different from that of patients with moderate/severe ARDS.
An electronic nose can rapidly and non-invasively discriminate between patients with and without ARDS with modest accuracy. Diagnostic accuracy increased when only moderate and severe ARDS patients were considered. This implicates that breath analysis may allow for rapid, bedside detection of ARDS, especially if our findings are reproduced using continuous exhaled breath profiling.
NTR2750, registered 11 February 2011.
急性呼吸窘迫综合征(ARDS)是一种常见的、严重的危重病并发症,其特征是肺部损伤和炎症。临床诊断可以通过客观的生物学标志物得到改善。电子鼻(eNose)技术可以快速、无创地提供呼气中的挥发性代谢物的呼吸图谱。我们假设呼吸图谱可以帮助准确诊断插管和机械通气的重症监护病房(ICU)患者的 ARDS。
前瞻性单中心队列研究,具有培训和时间外部验证队列。在入院后 24 小时内,使用电子鼻分析新插管和机械通气的 ICU 患者的呼吸。ARDS 按柏林临床共识定义进行诊断和分类。eNose 经过培训以识别培训队列中的 ARDS,并在时间外部验证队列中评估诊断性能。
在训练队列(40 例 ARDS 患者与 66 例对照)中,ARDS 的诊断模型显示出中等的鉴别能力,其接受者操作特征曲线(ROC-AUC)为 0.72(95%-置信区间(CI):0.63-0.82)。在外部验证队列(18 例 ARDS 患者与 26 例对照)中,AUC-ROC 为 0.71 [95%-CI:0.54-0.87]。将鉴别仅限于中度或重度 ARDS 患者与对照时,AUC-ROC 为 0.80 [95%-CI:0.70-0.90]。心肺水肿和肺炎患者的呼气谱与中重度 ARDS 患者不同。
电子鼻可以快速、无创地以中等准确度区分 ARDS 患者和非 ARDS 患者。当仅考虑中度和重度 ARDS 患者时,诊断准确性提高。这意味着呼吸分析可能允许快速、床边检测 ARDS,特别是如果使用连续呼气呼吸谱分析再现我们的结果。
NTR2750,于 2011 年 2 月 11 日注册。