Kaufman Peter A, Bloom Kenneth J, Burris Howard, Gralow Julie R, Mayer Musa, Pegram Mark, Rugo Hope S, Swain Sandra M, Yardley Denise A, Chau Miu, Lalla Deepa, Yoo Bongin, Brammer Melissa G, Vogel Charles L
Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire.
Cancer. 2014 Sep 1;120(17):2657-64. doi: 10.1002/cncr.28710. Epub 2014 Jun 13.
The importance of human epidermal growth factor receptor 2 (HER2) as a prognostic and predictive marker in invasive breast cancer is well established. Accurate assessment of HER2 status is essential to determine optimal treatment options.
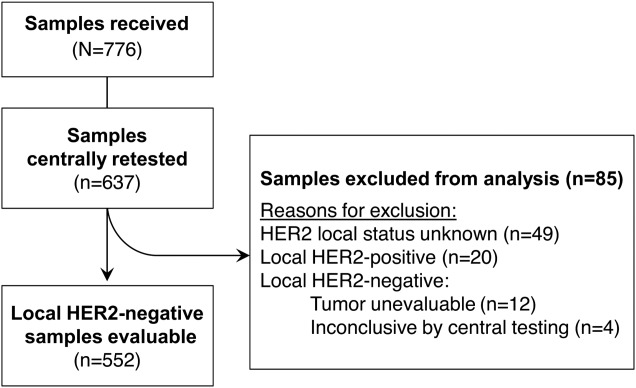
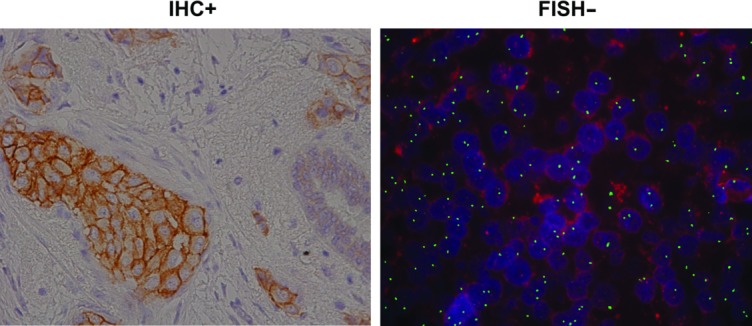
Breast cancer tumor tissue samples from the VIRGO observational cohort tissue substudy that were locally HER2-negative were retested centrally with both US Food and Drug Administration (FDA)-approved immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH) assays, using FDA-approved assay cutoffs; results were compared.
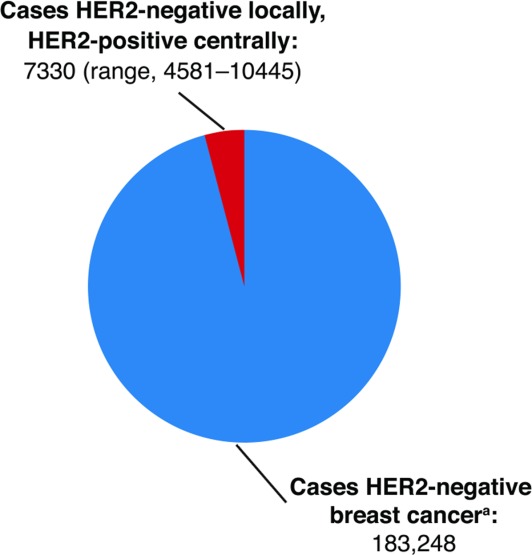
Of the 552 unique patient samples centrally retested with local HER2-negative results recorded, tumor samples from 22 (4.0%) patients were determined to be HER2-positive (95% confidence interval [CI] = 2.5%-5.7%). Of these, 18 had been tested locally by only one testing methodology; 15 of 18 were HER2-positive after the central retesting, based on the testing methodology not performed locally. Compared with the 530 patients with centrally confirmed HER2-negative tumors, the 22 patients with centrally determined HER2-positive tumors were younger (median age 56.5 versus 60.0 years) and more likely to have ER/PR-negative tumors (27.3% versus 22.3%). These patients also had shorter median progression-free survival (6.4 months [95% CI = 3.8-15.9 months] versus 9.1 months [95% CI = 8.3-10.3 months]) and overall survival (25.9 months [95% CI = 13.8-not estimable] versus 27.9 months [95% CI = 25.0-32.9 months]).
This study highlights the limitations of employing just one HER2 testing methodology in current clinical practice. It identifies a cohort of patients who did not receive potentially efficacious therapy because their tumor HER2-positivity was not determined by the test initially used. Because of inherent limitations in testing methodologies, it is inadvisable to rely on a single test to rule out potential benefit from HER2-targeted therapy.
人表皮生长因子受体2(HER2)作为浸润性乳腺癌的预后和预测标志物,其重要性已得到充分确立。准确评估HER2状态对于确定最佳治疗方案至关重要。
对VIRGO观察性队列组织子研究中局部HER2阴性的乳腺癌肿瘤组织样本,采用美国食品药品监督管理局(FDA)批准的免疫组织化学(IHC)和荧光原位杂交(FISH)检测方法进行中心重新检测,并采用FDA批准的检测临界值;对结果进行比较。
在552份中心重新检测的、记录为局部HER2阴性的独特患者样本中,22例(4.0%)患者的肿瘤样本被确定为HER2阳性(95%置信区间[CI]=2.5%-5.7%)。其中,18例仅通过一种检测方法进行了局部检测;在18例中,15例根据未在当地进行的检测方法,在中心重新检测后为HER2阳性。与530例中心确认HER2阴性肿瘤的患者相比,22例中心确定HER2阳性肿瘤的患者更年轻(中位年龄56.5岁对60.0岁),且更可能患有ER/PR阴性肿瘤(27.3%对22.3%)。这些患者的中位无进展生存期(6.4个月[95%CI=3.8-15.9个月]对9.1个月[95%CI=8.3-10.3个月])和总生存期(25.9个月[95%CI=13.8-不可估计]对27.9个月[95%CI=25.0-32.9个月])也更短。
本研究强调了当前临床实践中仅采用一种HER2检测方法的局限性。它识别出了一组患者,这些患者因最初使用的检测未确定其肿瘤HER2阳性而未接受可能有效的治疗。由于检测方法存在固有局限性,依靠单一检测来排除HER2靶向治疗的潜在益处是不可取的。