Khandaker Gulam, Zurynski Yvonne, Ridley Greta, Buttery Jim, Marshall Helen, Richmond Peter C, Royle Jenny, Gold Michael, Walls Tony, Whitehead Bruce, McIntyre Peter, Wood Nicholas, Booy Robert, Elliott Elizabeth J
The Discipline of Paediatrics and Child Health, The University of Sydney, Sydney, NSW, Australia; National Centre for Immunisation Research and Surveillance of Vaccine Preventable Diseases, The Children's Hospital at Westmead, Sydney, NSW, Australia; The Marie Bashir Institute for Infectious Diseases and Biosecurity (MBI), Sydney Medical School, the University of Sydney, Sydney, NSW, Australia.
Influenza Other Respir Viruses. 2014 Nov;8(6):636-45. doi: 10.1111/irv.12286. Epub 2014 Sep 27.
There are few large-scale, prospective studies of influenza A(H1N1)pdm09 in children that identify predictors of adverse outcomes.
We aimed to examine clinical epidemiology and predictors for adverse outcomes in children hospitalised with influenza A(H1N1)pdm09 in Australia.
Active hospital surveillance in six tertiary paediatric referral centres (June-September, 2009). All children aged <15 years admitted with laboratory-confirmed influenza A(H1N1)pdm09 were studied.
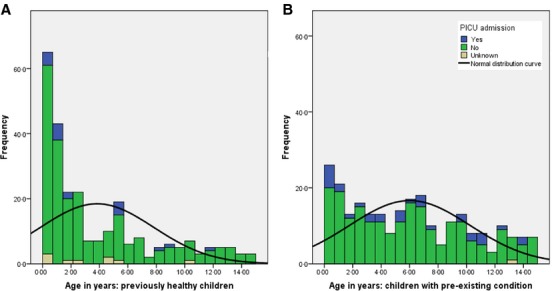
Of 601 children admitted with laboratory-confirmed influenza, 506 (84·2%) had influenza A(H1N1)pdm09. Half (51·0%) of children with influenza A(H1N1)pdm09 were previously healthy. Hospital stay was longer in children with pre-existing condition (mean 6·9 versus 4·9 days; P = 0·02) as was paediatric intensive care unit (PICU) stay (7·0 versus 2·3 days; P = 0·005). Rapid diagnosis decreased both antibiotic use and length of hospital and PICU stay. Fifty (9·9%) children were admitted to a PICU, 30 (5·9%) required mechanical ventilation and 5 (0·9%) died. Laboratory-proven bacterial co-infection and chronic lung disease were significant independent predictors of PICU admission (OR 6·89, 95% CI 3·15-15·06 and OR 3·58, 95% CI 1·41-9·07, respectively) and requirement for ventilation (OR 5·61, 95% CI 2·2-14·28 and OR 5·18, 95% CI 1·8-14·86, respectively). Chronic neurological disease was a predictor of admission to PICU (OR 2·30, 95% CI 1·14-4·61).
During the 2009 pandemic, influenza was a major cause of hospitalisation in tertiary paediatric hospitals. Co-infection and underlying chronic disease increased risk of PICU admission and/or ventilation. Half the children admitted were previously healthy, supporting a role for universal influenza vaccination in children.
针对甲型H1N1流感大流行病毒(A(H1N1)pdm09)感染儿童的大规模前瞻性研究较少,尚无关于不良结局预测因素的研究。
我们旨在研究澳大利亚因甲型H1N1流感大流行病毒(A(H1N1)pdm09)住院儿童的临床流行病学特征及不良结局的预测因素。
在六家三级儿科转诊中心开展主动监测(2009年6月至9月)。对所有年龄<15岁、实验室确诊为甲型H1N1流感大流行病毒(A(H1N1)pdm09)感染的住院儿童进行研究。
在601例实验室确诊流感的住院儿童中,506例(84.2%)为甲型H1N1流感大流行病毒(A(H1N1)pdm09)感染。一半(51.0%)感染甲型H1N1流感大流行病毒(A(H1N1)pdm09)的儿童既往健康。有基础疾病的儿童住院时间更长(平均6.9天对4.9天;P = 0.02),入住儿科重症监护病房(PICU)的时间也更长(7.0天对2.3天;P = 0.005)。快速诊断可减少抗生素使用以及缩短住院和入住PICU的时间。50例(9.9%)儿童入住PICU,30例(5.9%)需要机械通气,5例(0.9%)死亡。实验室确诊的细菌合并感染和慢性肺病是入住PICU(比值比[OR] 6.89,95%置信区间[CI] 3.15 - 15.06和OR 3.58,95% CI 1.41 - 9.07,分别)及需要机械通气(OR 5.61,95% CI = 2.2 - 14.28和OR 5.18,95% CI 1.8 - 14.86,分别)的显著独立预测因素。慢性神经疾病是入住PICU的预测因素(OR 2.30,95% CI 1.14 - 4.61)。
在2009年大流行期间,流感是三级儿科医院住院的主要原因。合并感染和潜在慢性疾病增加了入住PICU和/或进行机械通气的风险。一半住院儿童既往健康,这支持了儿童普遍接种流感疫苗的作用。