Stuckey Erin M, Stevenson Jennifer, Galactionova Katya, Baidjoe Amrish Y, Bousema Teun, Odongo Wycliffe, Kariuki Simon, Drakeley Chris, Smith Thomas A, Cox Jonathan, Chitnis Nakul
Department of Epidemiology and Public Health, Swiss Tropical and Public Health Institute, Basel, Switzerland; University of Basel, Basel, Switzerland.
Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom; Centre for Global Health Research, Kenya Medical Research Institute/Centers for Disease Control and Prevention, Kisumu, Kenya; Johns Hopkins Malaria Research Institute, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
PLoS One. 2014 Oct 7;9(10):e107700. doi: 10.1371/journal.pone.0107700. eCollection 2014.
Tools that allow for in silico optimization of available malaria control strategies can assist the decision-making process for prioritizing interventions. The OpenMalaria stochastic simulation modeling platform can be applied to simulate the impact of interventions singly and in combination as implemented in Rachuonyo South District, western Kenya, to support this goal.
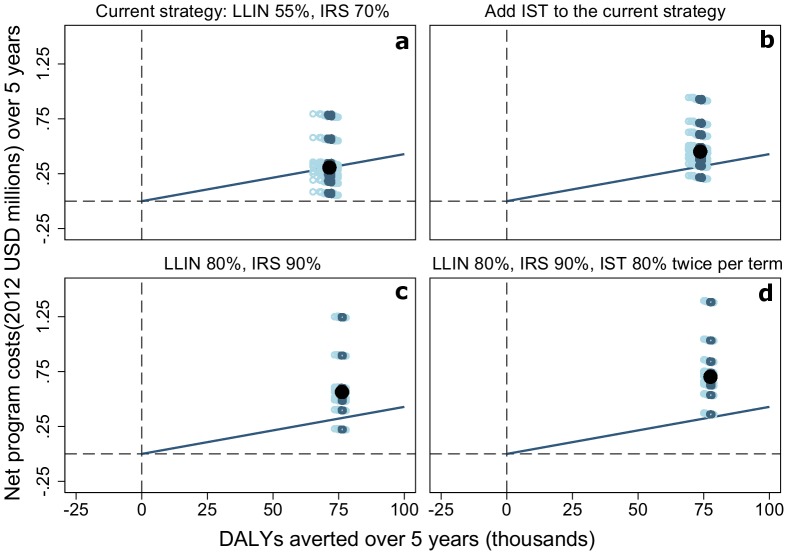
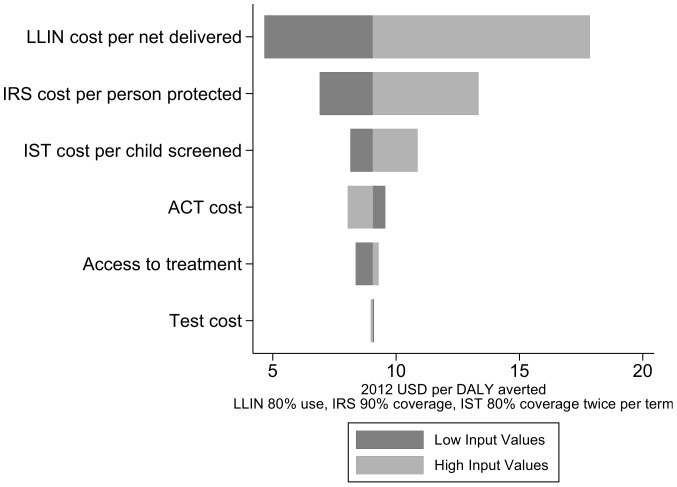
Combinations of malaria interventions were simulated using a previously-published, validated model of malaria epidemiology and control in the study area. An economic model of the costs of case management and malaria control interventions in Kenya was applied to simulation results and cost-effectiveness of each intervention combination compared to the corresponding simulated outputs of a scenario without interventions. Uncertainty was evaluated by varying health system and intervention delivery parameters.
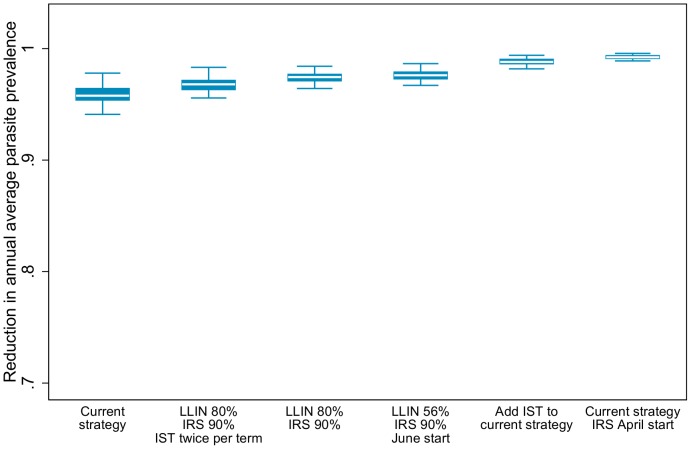
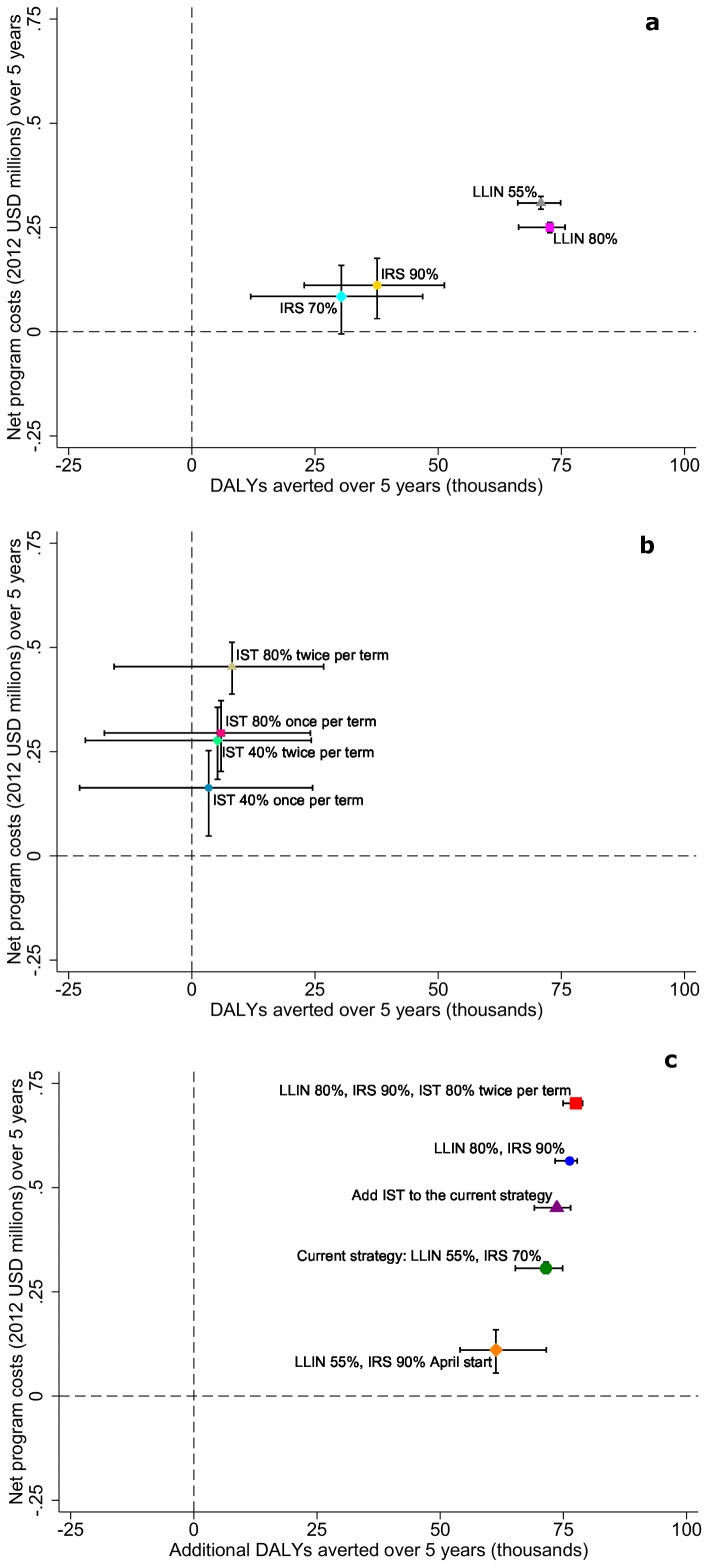
The intervention strategy with the greatest simulated health impact employed long lasting insecticide treated net (LLIN) use by 80% of the population, 90% of households covered by indoor residual spraying (IRS) with deployment starting in April, and intermittent screen and treat (IST) of school children using Artemether lumefantrine (AL) with 80% coverage twice per term. However, the current malaria control strategy in the study area including LLIN use of 56% and IRS coverage of 70% was the most cost effective at reducing disability-adjusted life years (DALYs) over a five year period.
All the simulated intervention combinations can be considered cost effective in the context of available resources for health in Kenya. Increasing coverage of vector control interventions has a larger simulated impact compared to adding IST to the current implementation strategy, suggesting that transmission in the study area is not at a level to warrant replacing vector control to a school-based screen and treat program. These results have the potential to assist malaria control program managers in the study area in adding new or changing implementation of current interventions.
能够对现有的疟疾控制策略进行计算机模拟优化的工具,有助于为干预措施的优先排序提供决策依据。开放疟疾随机模拟建模平台可用于单独或组合模拟肯尼亚西部拉楚奥尼奥南区实施的干预措施的影响,以支持这一目标。
使用先前发表并经过验证的该研究区域疟疾流行病学和控制模型,对疟疾干预措施的组合进行模拟。将肯尼亚病例管理和疟疾控制干预措施成本的经济模型应用于模拟结果,并将每种干预措施组合的成本效益与无干预情景下相应的模拟产出进行比较。通过改变卫生系统和干预措施实施参数来评估不确定性。
模拟显示对健康影响最大的干预策略是,80%的人口使用长效驱虫蚊帐(LLIN),90%的家庭进行室内滞留喷洒(IRS)且4月开始实施,以及对在校儿童采用蒿甲醚-本芴醇(AL)进行间歇性筛查和治疗(IST),每学期覆盖80%的儿童两次。然而,研究区域当前的疟疾控制策略,即长效驱虫蚊帐使用率为56%,室内滞留喷洒覆盖率为70%,在五年内减少伤残调整生命年(DALY)方面是最具成本效益的。
在肯尼亚现有的卫生资源背景下,所有模拟的干预措施组合都可被视为具有成本效益。与在当前实施策略中增加间歇性筛查和治疗相比,扩大病媒控制干预措施的覆盖率具有更大的模拟影响,这表明研究区域的传播水平尚不足以支持将病媒控制替换为基于学校的筛查和治疗方案。这些结果有可能帮助研究区域的疟疾控制项目管理人员增加新的干预措施或改变当前干预措施的实施方式。