Brown C Hendricks, Chamberlain Patricia, Saldana Lisa, Padgett Courtenay, Wang Wei, Cruden Gracelyn
Department of Psychiatry and Behavioral Sciences, Northwestern University Feinberg School of Medicine, 750 North Lake Shore Dr, 10th Floor, Chicago, IL, 60611, USA.
Oregon Social Learning Center, 10 Shelton Mcmurphey Blvd, Eugene, OR, 97401, USA.
Implement Sci. 2014 Oct 14;9:134. doi: 10.1186/s13012-014-0134-8.
Much is to be learned about what implementation strategies are the most beneficial to communities attempting to adopt evidence-based practices. This paper presents outcomes from a randomized implementation trial of Multidimensional Treatment Foster Care (MTFC) in child public service systems in California and Ohio, including child welfare, juvenile justice, and mental health.
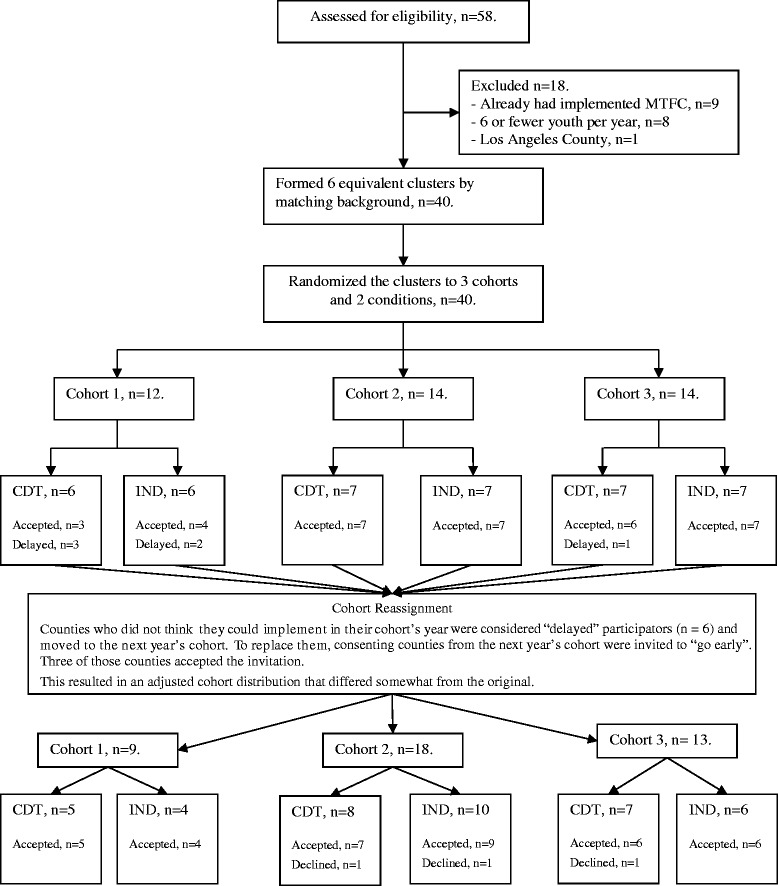
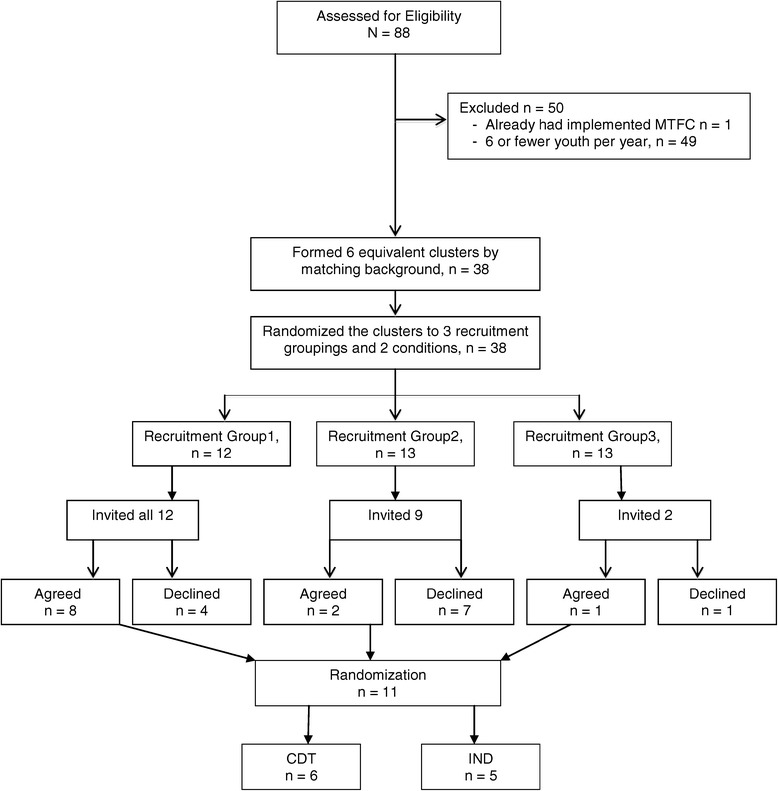
Fifty-one counties were assigned randomly to one of two different implementation strategies (Community Development Teams (CDT) or independent county implementation strategy (IND)) across four cohorts after being matched on county characteristics. We compared these two strategies on implementation process, quality, and milestone achievements using the Stages of Implementation Completion (SIC) (Implement Sci 6(1):1-8, 2011).
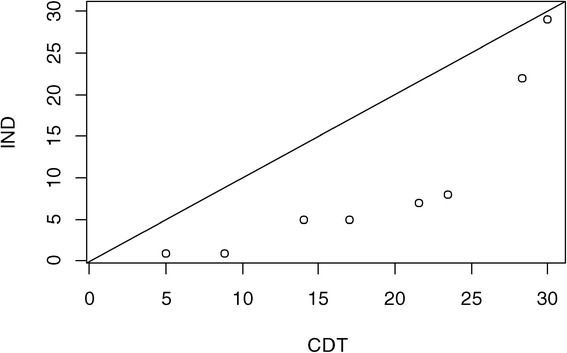
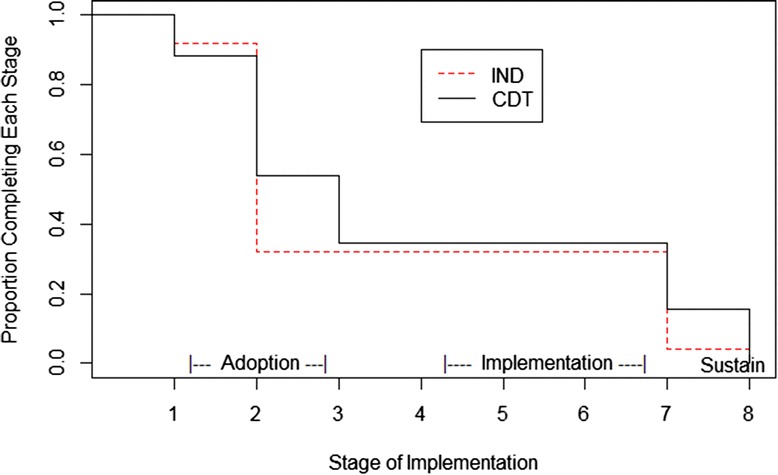
A composite score for each county, combining the final implementation stage attained, the number of families served, and quality of implementation, was used as the primary outcome. No significant difference between CDT and IND was found for the composite measure. Additional analyses showed that there was no evidence that CDT increased the proportion of counties that started-up programs (i.e., placed at least one family in MTFC). For counties that did implement MTFC, those in the CDT condition served over twice as many youth during the study period as did IND. Of the counties that successfully achieved program start-up, those in the CDT condition completed the implementation process more thoroughly, as measured by the SIC. We found no significant differences by implementation condition on the time it took for first placement, achieving competency, or number of stages completed.
This trial did not lead to higher rates of implementation or faster implementation but did provide evidence for more robust implementation in the CDT condition compared to IND implementation once the first family received MTFC services. This trial was successful from a design perspective in that no counties dropped out, even though this study took place during an economic recession. We believe that this methodologic approach of measurement utilizing the SIC, which is comprised of the three dimensions of quality, quantity, and timing, is appropriate for a wide range of implementation and translational studies.
Trial ID: NCT00880126 (ClinicalTrials.gov).
对于哪些实施策略对试图采用循证实践的社区最为有益,仍有许多有待了解之处。本文介绍了在加利福尼亚州和俄亥俄州儿童公共服务系统(包括儿童福利、青少年司法和心理健康系统)中进行的多维治疗寄养(MTFC)随机实施试验的结果。
在根据县特征进行匹配后,51个县被随机分配到四个队列中的两种不同实施策略之一(社区发展团队(CDT)或独立县实施策略(IND))。我们使用实施完成阶段(SIC)(《实施科学》6(1):1 - 8, 2011)比较了这两种策略在实施过程、质量和里程碑成就方面的情况。
每个县的综合得分,结合最终达到的实施阶段、服务的家庭数量和实施质量,被用作主要结果。在综合指标上,未发现CDT和IND之间存在显著差异。进一步分析表明,没有证据表明CDT增加了启动项目的县的比例(即至少安置一个家庭接受MTFC)。对于确实实施了MTFC的县,在研究期间,处于CDT条件下的县服务的青少年数量是IND条件下的两倍多。在成功实现项目启动的县中,根据SIC衡量,处于CDT条件下的县更彻底地完成了实施过程。我们发现在首次安置时间、达到胜任能力的时间或完成的阶段数量方面,实施条件之间没有显著差异。
该试验并未导致更高的实施率或更快的实施速度,但确实提供了证据表明,与IND实施相比,一旦第一个家庭接受MTFC服务,在CDT条件下的实施更为稳健。从设计角度来看,该试验是成功的,因为即使这项研究是在经济衰退期间进行的,也没有县退出。我们认为,这种利用SIC进行测量的方法学方法,由质量、数量和时间三个维度组成,适用于广泛的实施和转化研究。
试验编号:NCT00880126(ClinicalTrials.gov)。