Jee Tae Keun, Lee Sun-Ho, Kim Eun-Sang, Eoh Whan
Department of Neurosurgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
J Korean Neurosurg Soc. 2014 Aug;56(2):162-5. doi: 10.3340/jkns.2014.56.2.162. Epub 2014 Aug 31.
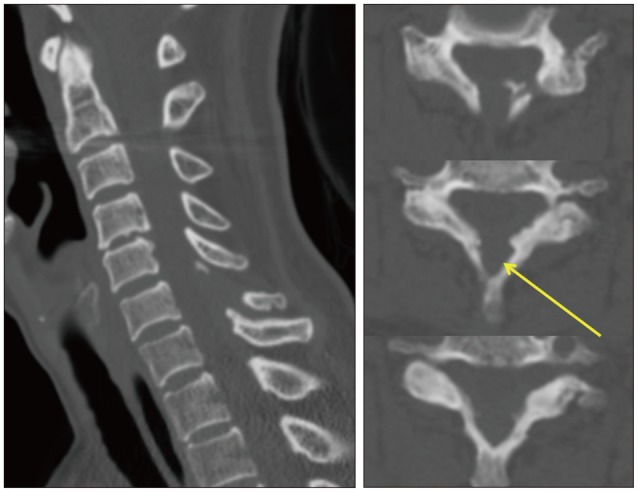
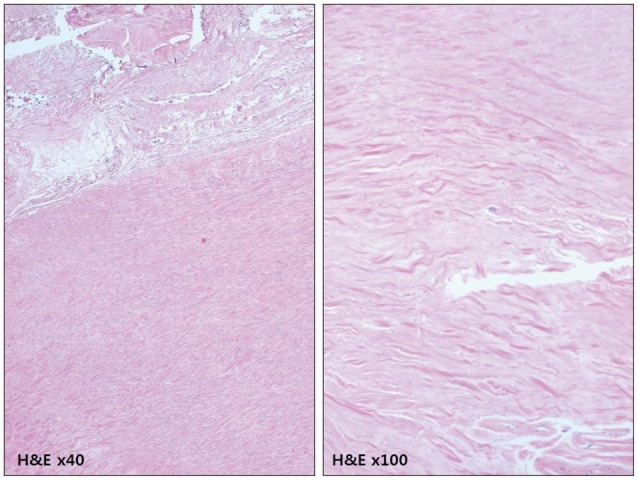
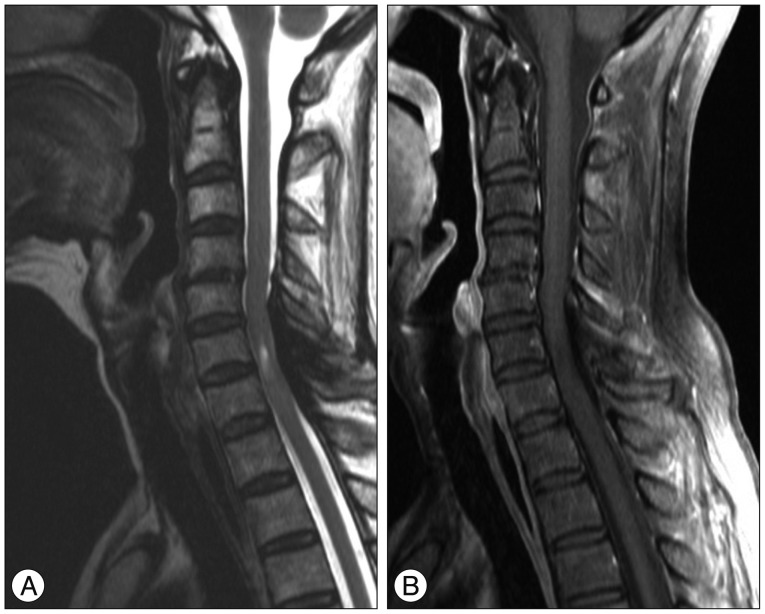
Idiopathic hypertrophic spinal pachymeningitis (IHSP) is a chronic, progressive, inflammatory disorder characterized by marked fibrosis of the spinal dura mater with unknown etiology. According to the location of the lesion, it might induce neurologic deficits by compression of spinal cord and nerve root. A 58-year old female with a 3-year history of progressive weakness in both lower extremities was referred to our institute. Spinal computed tomography (CT) scan showed an osteolytic lesion involving base of the C6 spinous process with adjacent epidural mass. Magnetic resonance imaging (MRI) revealed an epidural mass involving dorsal aspect of cervical spinal canal from C5 to C7 level, with low signal intensity on T1 and T2 weighted images and non-enhancement on T1 weighted-enhanced images. We decided to undertake surgical exploration. At the operation field, there was yellow colored, thickened fibrous tissue over the dura mater. The lesion was removed totally, and decompression of spinal cord was achieved. Symptoms improved partially after the operation. Histopathologically, fibrotic pachymeninges with scanty inflammatory cells was revealed, which was compatible with diagnosis of idiopathic hypertrophic pachymeningitis. Six months after operation, motor power grade of both lower extremities was normal on physical examination. However, the patient still complained of mild weakness in the right lower extremity. Although the nature of IHSP is generally indolent, decompressive surgery should be considered for the patient with definite or progressive neurologic symptoms in order to prevent further deterioration. In addition, IHSP can present as an osteolytic lesion. Differential diagnosis with neoplastic disease, including giant cell tumor, is important.
特发性肥厚性硬脊膜脑膜炎(IHSP)是一种慢性、进行性炎症性疾病,其特征为硬脊膜显著纤维化,病因不明。根据病变部位,它可能因压迫脊髓和神经根而导致神经功能缺损。一名58岁女性,有3年双下肢进行性无力病史,被转诊至我院。脊柱计算机断层扫描(CT)显示C6棘突基部有溶骨性病变及相邻硬膜外肿块。磁共振成像(MRI)显示硬膜外肿块累及C5至C7水平的颈段椎管背侧,在T1加权像和T2加权像上呈低信号强度,在T1加权增强像上无强化。我们决定进行手术探查。在手术区域,硬脊膜上有黄色增厚的纤维组织。病变被完全切除,脊髓得到减压。术后症状部分改善。组织病理学显示为纤维化硬脊膜,炎症细胞稀少,符合特发性肥厚性硬脊膜炎的诊断。术后6个月,体格检查双下肢肌力分级正常。然而,患者仍主诉右下肢轻度无力。尽管IHSP的病程通常较为缓慢,但对于有明确或进行性神经症状的患者,应考虑进行减压手术以防止病情进一步恶化。此外,IHSP可表现为溶骨性病变。与包括巨细胞瘤在内的肿瘤性疾病进行鉴别诊断很重要。