Kind Amy J H, Jencks Steve, Brock Jane, Yu Menggang, Bartels Christie, Ehlenbach William, Greenberg Caprice, Smith Maureen
Ann Intern Med. 2014 Dec 2;161(11):765-74. doi: 10.7326/M13-2946.
Measures of socioeconomic disadvantage may enable improved targeting of programs to prevent rehospitalizations, but obtaining such information directly from patients can be difficult. Measures of U.S. neighborhood socioeconomic disadvantage are more readily available but are rarely used clinically.
To evaluate the association between neighborhood socioeconomic disadvantage at the census block group level, as measured by the Singh validated area deprivation index (ADI), and 30-day rehospitalization.
Retrospective cohort study.
United States.
Random 5% national sample of Medicare patients discharged with congestive heart failure, pneumonia, or myocardial infarction between 2004 and 2009 (n = 255,744).
Medicare data were linked to 2000 census data to construct an ADI for each patient's census block group, which were then sorted into percentiles by increasing ADI. Relationships between neighborhood ADI grouping and 30-day rehospitalization were evaluated using multivariate logistic regression models, controlling for patient sociodemographic characteristics, comorbid conditions and severity, and index hospital characteristics.
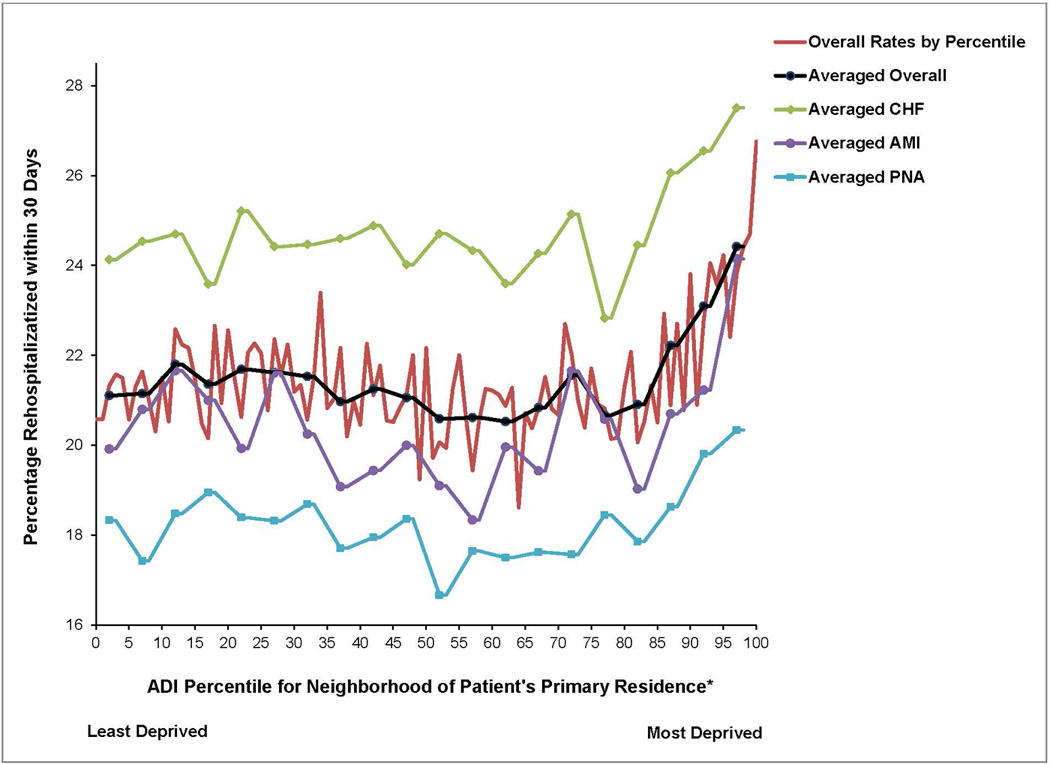
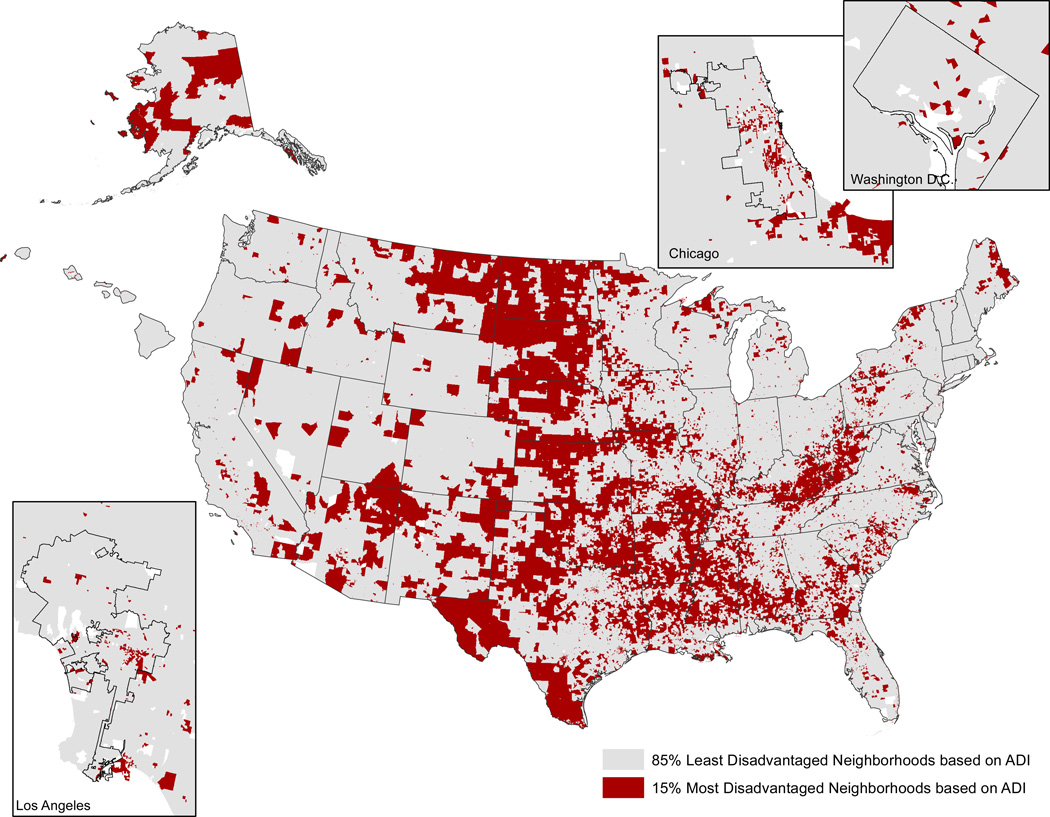
The 30-day rehospitalization rate did not vary significantly across the least disadvantaged 85% of neighborhoods, which had an average rehospitalization rate of 21%. However, within the most disadvantaged 15% of neighborhoods, rehospitalization rates increased from 22% to 27% with worsening ADI. This relationship persisted after full adjustment, with the most disadvantaged neighborhoods having a rehospitalization risk (adjusted risk ratio, 1.09 [95% CI, 1.05 to 1.12]) similar to that of chronic pulmonary disease (adjusted risk ratio, 1.06 [CI, 1.04 to 1.08]) and greater than that of uncomplicated diabetes (adjusted risk ratio, 0.95 [CI, 0.94 to 0.97]).
No direct markers of care quality or access.
Residence within a disadvantaged U.S. neighborhood is a rehospitalization predictor of magnitude similar to chronic pulmonary disease. Measures of neighborhood disadvantage, such as the ADI, could potentially be used to inform policy and care after hospital discharge.
National Institute on Aging and University of Wisconsin School of Medicine and Public Health's Institute for Clinical and Translational Research and Health Innovation Program.
社会经济劣势指标可能有助于改进预防再次住院项目的目标定位,但直接从患者那里获取此类信息可能很困难。美国邻里社会经济劣势指标更容易获得,但在临床中很少使用。
评估以辛格验证的区域剥夺指数(ADI)衡量的人口普查街区组层面的邻里社会经济劣势与30天再次住院之间的关联。
回顾性队列研究。
美国。
2004年至2009年间因充血性心力衰竭、肺炎或心肌梗死出院的医疗保险患者的5%全国随机样本(n = 255,744)。
医疗保险数据与2000年人口普查数据相链接,为每位患者的人口普查街区组构建一个ADI,然后按ADI递增顺序将其分为百分位数。使用多变量逻辑回归模型评估邻里ADI分组与30天再次住院之间的关系,同时控制患者的社会人口统计学特征、合并症情况和严重程度以及索引医院特征。
在最不具劣势的85%的邻里中,30天再次住院率没有显著差异,这些邻里的平均再次住院率为21%。然而,在最具劣势的15%的邻里中,随着ADI恶化,再次住院率从22%上升到27%。在完全调整后,这种关系仍然存在,最具劣势的邻里的再次住院风险(调整风险比,1.09 [95% CI,1.05至1.12])与慢性肺病的风险(调整风险比,1.06 [CI,1.04至1.08])相似,且高于单纯糖尿病的风险(调整风险比,0.95 [CI,0.94至0.97])。
没有护理质量或可及性的直接指标。
居住在美国劣势邻里中是一个与慢性肺病程度相似的再次住院预测因素。邻里劣势指标,如ADI,可能可用于为出院后的政策和护理提供信息。
美国国立衰老研究所以及威斯康星大学医学院和公共卫生学院的临床与转化研究及健康创新项目研究所。