Suh Joome, Sinclair Elizabeth, Peterson Julia, Lee Evelyn, Kyriakides Tassos C, Li Fang-Yong, Hagberg Lars, Fuchs Dietmar, Price Richard W, Gisslen Magnus, Spudich Serena
Yale School of Medicine, 367 Cedar Street, New Haven, CT 06510, USA.
Department of Medicine, UCSF School of Medicine, 1001 Potrero Avenue, SFGH 100, San Francisco, CA, 94143, USA.
J Neuroinflammation. 2014 Dec 3;11:199. doi: 10.1186/s12974-014-0199-y.
Central nervous system (CNS) inflammation is a mediator of brain injury in HIV infection. To study the natural course of CNS inflammation in the early phase of infection, we analyzed longitudinal levels of soluble and cellular markers of inflammation in cerebrospinal fluid (CSF) and blood, beginning with primary HIV-1 infection (PHI).
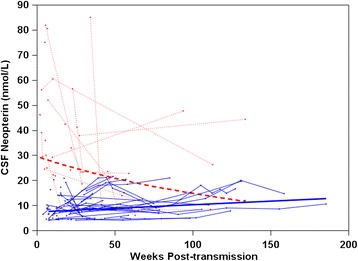
Antiretroviral-naïve subjects identified as having PHI (less than one year since HIV transmission) participated in phlebotomy and lumbar puncture at baseline and at variable intervals thereafter. Mixed-effects models were used to analyze longitudinal levels of CSF neopterin and percentages of activated cluster of differentiation (CD)4+ and CD8+ T-cells (co-expressing CD38 and human leukocyte antigen-D-related (HLA-DR)) in blood and CSF.
A total of 81 subjects were enrolled at an average of 100 days after HIV transmission and had an average follow-up period of 321 days, with the number of visits ranging from one to 13. At baseline, the majority of subjects had CSF neopterin concentrations above the upper limit of normal. The baseline concentration was associated with the longitudinal trajectory of CSF neopterin. In subjects with baseline levels of less than 21 nmol/L, a cutoff value obtained from a mixed-effects model, CSF neopterin increased by 2.9% per 10 weeks (n = 33; P <0.001), whereas it decreased by 6.7% in subjects with baseline levels of more than 21 nmol/L (n = 11; P = 0.001). In a subset with available flow cytometry data (n = 42), the percentages of activated CD4+ and CD8+ T-cells in CSF increased by 0.8 (P <0.001) and 0.73 (P = 0.02) per 10 weeks, respectively.
Neopterin levels and the percentages of activated CD4+ and CD8+ T-cells in CSF progressively increase in most subjects without treatment during early HIV-1 infection, suggesting an accrual of intrathecal inflammation, a major contributor to neuropathology in HIV infection.
中枢神经系统(CNS)炎症是HIV感染中脑损伤的介质。为了研究感染早期CNS炎症的自然病程,我们分析了从原发性HIV-1感染(PHI)开始的脑脊液(CSF)和血液中炎症的可溶性和细胞标志物的纵向水平。
被确定为患有PHI(自HIV传播以来不到一年)且未接受过抗逆转录病毒治疗的受试者在基线时以及此后的不同时间间隔接受静脉穿刺和腰椎穿刺。混合效应模型用于分析CSF新蝶呤的纵向水平以及血液和CSF中活化的分化簇(CD)4+和CD8+ T细胞(共表达CD38和人类白细胞抗原-D相关分子(HLA-DR))的百分比。
共有81名受试者在HIV传播后平均100天入组,平均随访期为321天,就诊次数从1次到13次不等。在基线时,大多数受试者的CSF新蝶呤浓度高于正常上限。基线浓度与CSF新蝶呤的纵向轨迹相关。在基线水平低于21 nmol/L(从混合效应模型获得的临界值)的受试者中,CSF新蝶呤每10周增加2.9%(n = 33;P <0.001),而在基线水平高于21 nmol/L的受试者中则下降6.7%(n = 11;P = 0.001)。在有可用流式细胞术数据的亚组(n = 42)中,CSF中活化的CD4+和CD8+ T细胞百分比每10周分别增加0.8(P <0.001)和0.73(P = 0.02)。
在早期HIV-1感染期间,大多数未经治疗的受试者CSF中的新蝶呤水平以及活化的CD4+和CD8+ T细胞百分比逐渐增加,提示鞘内炎症的累积,这是HIV感染神经病理学的主要促成因素。