Krist Alex H, Aycock Rebecca A, Etz Rebecca S, Devoe Jennifer E, Sabo Roy T, Williams Robert, Stein Karen L, Iwamoto Gary, Puro Jon, Deshazo Jon, Kashiri Paulette Lail, Arkind Jill, Romney Crystal, Kano Miria, Nelson Christine, Longo Daniel R, Wolver Susan, Woolf Steven H
Department of Family Medicine and Population Health, Virginia Commonwealth University, Richmond, VA, Virginia.
Implement Sci. 2014 Dec 11;9:181. doi: 10.1186/s13012-014-0181-1.
Evidence-based preventive services for early detection of cancer and other health conditions offer profound health benefits, yet Americans receive only half of indicated services. Policy initiatives promote the adoption of information technologies to engage patients in care. We developed a theory-driven interactive preventive health record (IPHR) to engage patients in health promotion. The model defines five levels of functionality: (1) collecting patient information, (2) integrating with electronic health records (EHRs), (3) translating information into lay language, (4) providing individualized, guideline-based clinical recommendations, and (5) facilitating patient action. It is hypothesized that personal health records (PHRs) with these higher levels of functionality will inform and activate patients in ways that simpler PHRs cannot. However, realizing this vision requires both technological advances and effective implementation based upon clinician and practice engagement.
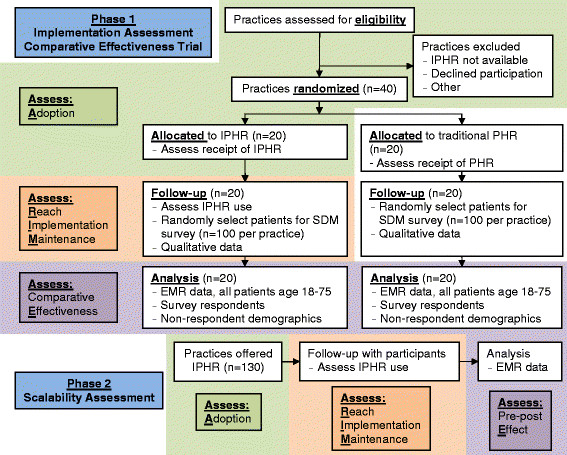
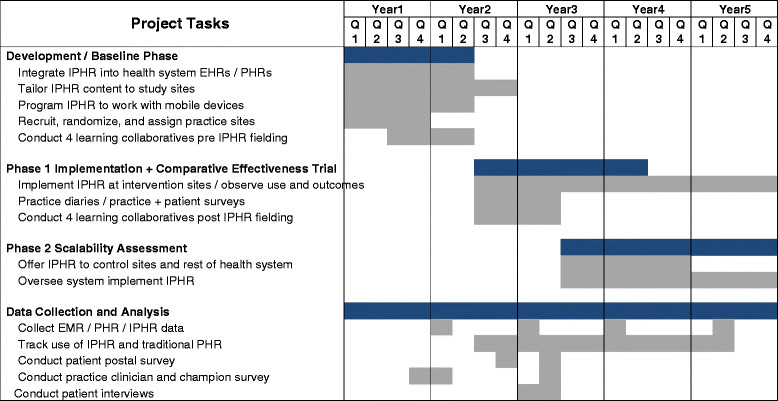
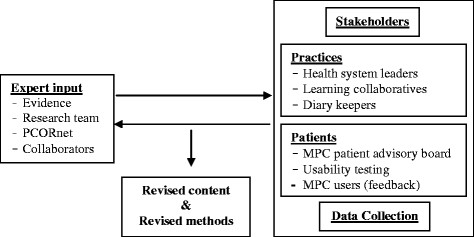
METHODS/DESIGN: We are starting a two-phase, mixed-method trial to evaluate whether the IPHR is scalable across a large number of practices and how its uptake differs for minority and disadvantaged patients. In phase 1, 40 practices from three practice-based research networks will be randomized to add IPHR functionality to their PHR versus continue to use their existing PHR. Throughout the study, we will engage intervention practices to locally tailor IPHR content and learn how to integrate new functions into their practice workflow. In phase 2, the IPHR to all nonintervention practices to observe whether the IPHR can be implemented more broadly (Scalability). Phase 1 will feature an implementation assessment in intervention practices, based on the RE-AIM model, to measure Reach (creation of IPHR accounts by patients), Adoption (practice decision to use the IPHR), Implementation (consistency, fidelity, barriers, and facilitators of use), and Maintenance (sustained use). The incremental effect of the IPHR on receipt of cancer screening tests and shared decision-making compared to traditional PHRs will assess Effectiveness. In phase 2, we will assess similar outcomes as phase 1 except for effectiveness.
This study will yield information about the effectiveness of new health information technologies designed to actively engage patients in their care as well as information about how to effectively implement and disseminate PHRs by engaging clinicians.
ClinicalTrials.gov: NCT02138448.
基于证据的癌症及其他健康状况早期检测预防性服务能带来巨大的健康益处,但美国人仅接受了一半的推荐服务。政策举措推动采用信息技术以使患者参与医疗。我们开发了一种理论驱动的交互式预防性健康记录(IPHR),以促使患者参与健康促进。该模型定义了五个功能级别:(1)收集患者信息;(2)与电子健康记录(EHR)集成;(3)将信息转化为通俗易懂的语言;(4)提供基于指南的个性化临床建议;(5)促进患者行动。据推测,具有这些更高功能级别的个人健康记录(PHR)将以更简单的PHR无法做到的方式告知并激励患者。然而,要实现这一愿景既需要技术进步,也需要基于临床医生和医疗机构参与的有效实施。
方法/设计:我们正在开展一项两阶段的混合方法试验,以评估IPHR能否在大量医疗机构中推广,以及少数族裔和弱势患者对其的接受情况有何不同。在第一阶段,来自三个基于医疗机构的研究网络的40家医疗机构将被随机分组,一组在其PHR中添加IPHR功能,另一组继续使用现有的PHR。在整个研究过程中,我们将促使参与干预的医疗机构根据当地情况调整IPHR内容,并学习如何将新功能融入其医疗工作流程。在第二阶段,将IPHR推广至所有未参与干预的医疗机构,以观察IPHR能否更广泛地实施(可扩展性)。第一阶段将基于RE-AIM模型对参与干预的医疗机构进行实施评估,以衡量覆盖范围(患者创建IPHR账户的情况)、采用情况(医疗机构决定使用IPHR)、实施情况(使用的一致性、保真度、障碍和促进因素)以及维持情况(持续使用)。与传统PHR相比,IPHR对接受癌症筛查测试和共同决策的增量影响将评估其有效性。在第二阶段,我们将评估与第一阶段类似的结果,但不包括有效性。
本研究将提供有关旨在积极促使患者参与医疗的新型健康信息技术有效性的信息,以及有关如何通过促使临床医生参与来有效实施和推广PHR的信息。
ClinicalTrials.gov:NCT02138448。