Arsenijevic Jelena, Tummers Lars, Bosma Niels
Utrecht University School of Governance, Faculty of Law Economics and Governance, Utrecht, Netherlands.
Utrecht University School of Economics, Faculty of Law Economics and Governance, Utrecht, Netherlands.
J Med Internet Res. 2020 Feb 6;22(2):e11613. doi: 10.2196/11613.
Electronic health (eHealth) tools are increasingly being applied in health care. They are expected to improve access to health care, quality of health care, and health outcomes. Although the advantages of using these tools in health care are well described, it is unknown to what extent eHealth tools are effective when used by vulnerable population groups, such as the elderly, people with low socioeconomic status, single parents, minorities, or immigrants.
This study aimed to examine whether the design and implementation characteristics of eHealth tools contribute to better use of these tools among vulnerable groups.
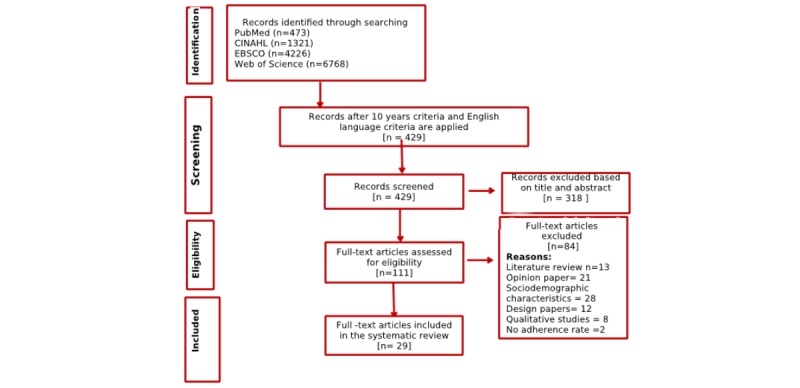
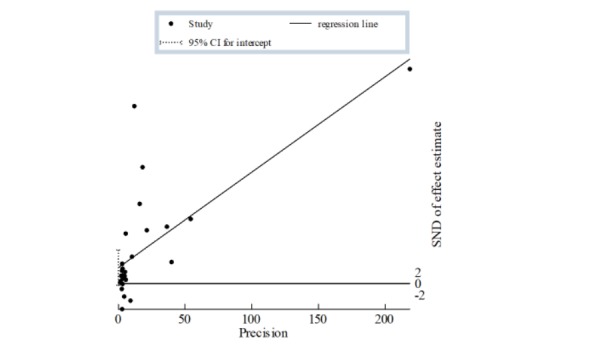
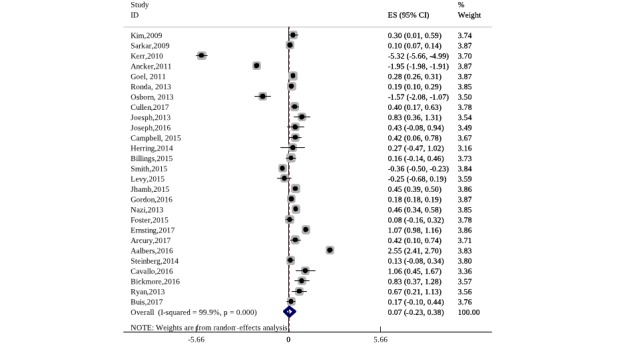
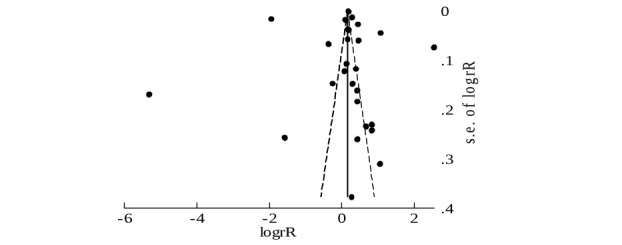
In this systematic review, we assessed the design and implementation characteristics of eHealth tools that are used by vulnerable groups. In the meta-analysis, we used the adherence rate as an effect size measure. The adherence rate is defined as the number of people who are repetitive users (ie, use the eHealth tool more than once). We also performed a meta-regression analysis to examine how different design and implementation characteristics influenced the adherence rate.
Currently, eHealth tools are continuously used by vulnerable groups but to a small extent. eHealth tools that use multimodal content (such as videos) and have the possibility for direct communication with providers show improved adherence among vulnerable groups.
eHealth tools that use multimodal content and provide the possibility for direct communication with providers have a higher adherence among vulnerable groups. However, most of the eHealth tools are not embedded within the health care system. They are usually focused on specific problems, such as diabetes or obesity. Hence, they do not provide comprehensive services for patients. This limits the use of eHealth tools as a replacement for existing health care services.
电子健康(eHealth)工具在医疗保健领域的应用日益广泛。人们期望这些工具能改善医疗保健的可及性、质量以及健康结局。尽管在医疗保健中使用这些工具的优势已得到充分描述,但对于弱势群体(如老年人、社会经济地位较低者、单亲父母、少数族裔或移民)使用eHealth工具的有效性程度尚不清楚。
本研究旨在探讨eHealth工具的设计和实施特征是否有助于弱势群体更好地使用这些工具。
在这项系统评价中,我们评估了弱势群体使用的eHealth工具的设计和实施特征。在荟萃分析中,我们将依从率作为效应量指标。依从率定义为重复使用者(即使用eHealth工具不止一次)的人数。我们还进行了荟萃回归分析,以研究不同的设计和实施特征如何影响依从率。
目前,弱势群体持续使用eHealth工具,但使用程度较低。使用多模态内容(如视频)且有可能与提供者直接沟通的eHealth工具在弱势群体中的依从性有所提高。
使用多模态内容并提供与提供者直接沟通可能性的eHealth工具在弱势群体中的依从性较高。然而,大多数eHealth工具并未嵌入医疗保健系统。它们通常专注于特定问题,如糖尿病或肥胖症。因此,它们无法为患者提供全面的服务。这限制了eHealth工具替代现有医疗保健服务的使用。