Rosa Ghislaine, Huaylinos Maria L, Gil Ana, Lanata Claudio, Clasen Thomas
Faculty of Infectious and Tropical Diseases, London School of Hygiene & Tropical Medicine, London, United Kingdom.
Instituto de Investigación Nutricional, Lima, Peru.
PLoS One. 2014 Dec 18;9(12):e114997. doi: 10.1371/journal.pone.0114997. eCollection 2014.
Household water treatment (HWT) can improve drinking water quality and prevent disease if used correctly and consistently by vulnerable populations. Over 1.1 billion people report treating their water prior to drinking it. These estimates, however, are based on responses to household surveys that may exaggerate the consistency and microbiological performance of the practice-key factors for reducing pathogen exposure and achieving health benefits. The objective of this study was to examine how HWT practices are actually performed by households identified as HWT users, according to international monitoring standards.
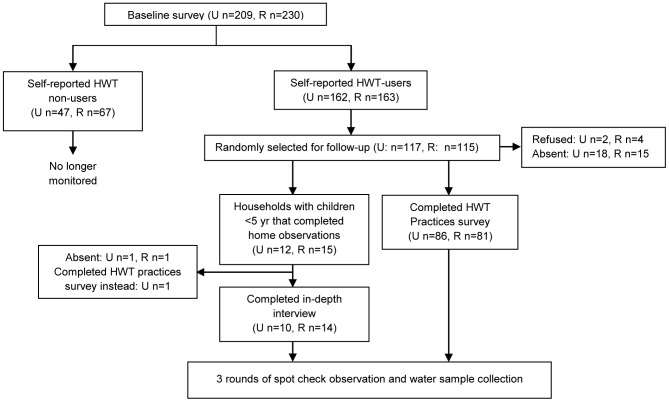
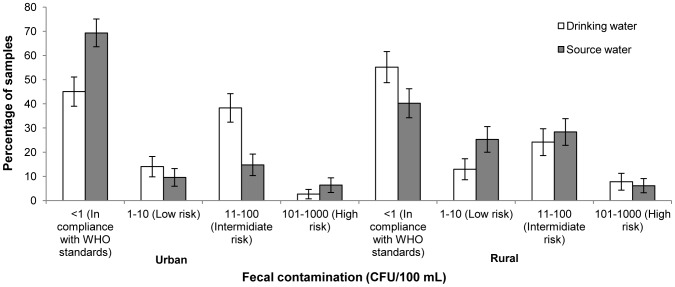
We conducted a 6-month case study in urban (n = 117 households) and rural (n = 115 households) Peru, a country in which 82.8% of households report treating their water at home. We used direct observation, in-depth interviews, surveys, spot-checks, and water sampling to assess water treatment practices among households that claimed to treat their drinking water at home. While consistency of reported practices was high in both urban (94.8%) and rural (85.3%) settings, availability of treated water (based on self-report) at time of collection was low, with 67.1% and 23.0% of urban and rural households having treated water at all three sampling visits. Self-reported consumption of untreated water in the home among adults and children <5 was common and this was corroborated during home observations. Drinking water of self-reported users was significantly better than source water in the urban setting and negligible but significantly better in the rural setting. However, only 46.3% and 31.6% of households had drinking water <1 CFU/100 mL at all follow-up visits.
Our results raise questions about the usefulness of current international monitoring of HWT practices and their usefulness as a proxy indicator for drinking water quality. The lack of consistency and sub-optimal microbiological effectiveness also raises questions about the potential of HWT to prevent waterborne diseases.
如果弱势群体正确且持续地使用家庭水处理(HWT),则可改善饮用水质量并预防疾病。超过11亿人报告称在饮用前会对水进行处理。然而,这些估计是基于家庭调查的回应,而这些回应可能夸大了这种做法的一致性和微生物学效果,而这两个因素对于减少病原体暴露和实现健康益处至关重要。本研究的目的是根据国际监测标准,研究被认定为家庭水处理使用者的家庭实际是如何进行家庭水处理的。
我们在秘鲁的城市(n = 117户家庭)和农村(n = 115户家庭)开展了一项为期6个月的案例研究,秘鲁有82.8%的家庭报告称在家中对水进行处理。我们采用直接观察、深入访谈、调查、抽查和水样采集等方法,来评估那些声称在家中处理饮用水的家庭的水处理做法。虽然在城市(94.8%)和农村(85.3%)地区,报告的做法的一致性都很高,但在采集水样时,(根据自我报告)经处理的水的可得性较低,城市和农村家庭在全部三次采样时都有经处理水的比例分别为67.1%和23.0%。在成年人和5岁以下儿童中,家中自报饮用未处理水的情况很常见,这在家庭观察中得到了证实。在城市地区,自我报告的使用者的饮用水明显优于水源水,在农村地区,虽然差异可忽略不计,但也明显更好。然而,在所有后续访问中,只有46.3%和31.6%的家庭的饮用水<1 CFU/100 mL。
我们的研究结果对当前国际上对家庭水处理做法的监测的有用性及其作为饮用水质量替代指标的有用性提出了质疑。缺乏一致性和微生物学效果欠佳也对家庭水处理预防水传播疾病的潜力提出了质疑。