Kiguli Sarah, Maitland Kathryn, George Elizabeth C, Olupot-Olupot Peter, Opoka Robert O, Engoru Charles, Akech Samuel O, Nyeko Richard, Mtove George, Reyburn Hugh, Levin Michael, Babiker Abdel G, Gibb Diana M, Crawley Jane
Kilifi Clinical Trials Facility, KEMRI-Wellcome Trust Research Programme, Nairobi, Kenya.
BMC Med. 2015 Feb 2;13:21. doi: 10.1186/s12916-014-0246-7.
Severe anaemia in children is a leading cause of hospital admission and a major cause of mortality in sub-Saharan Africa, yet there are limited published data on blood transfusion in this vulnerable group.
We present data from a large controlled trial of fluid resuscitation (Fluid Expansion As Supportive Therapy (FEAST) trial) on the prevalence, clinical features, and transfusion management of anaemia in children presenting to hospitals in three East African countries with serious febrile illness (predominantly malaria and/or sepsis) and impaired peripheral perfusion.
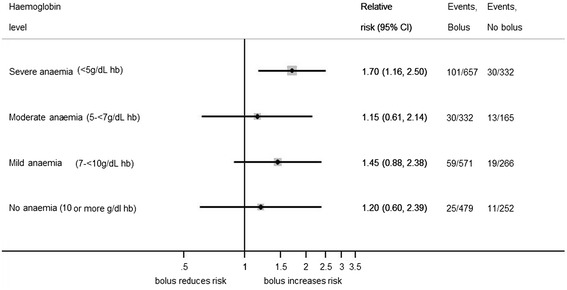
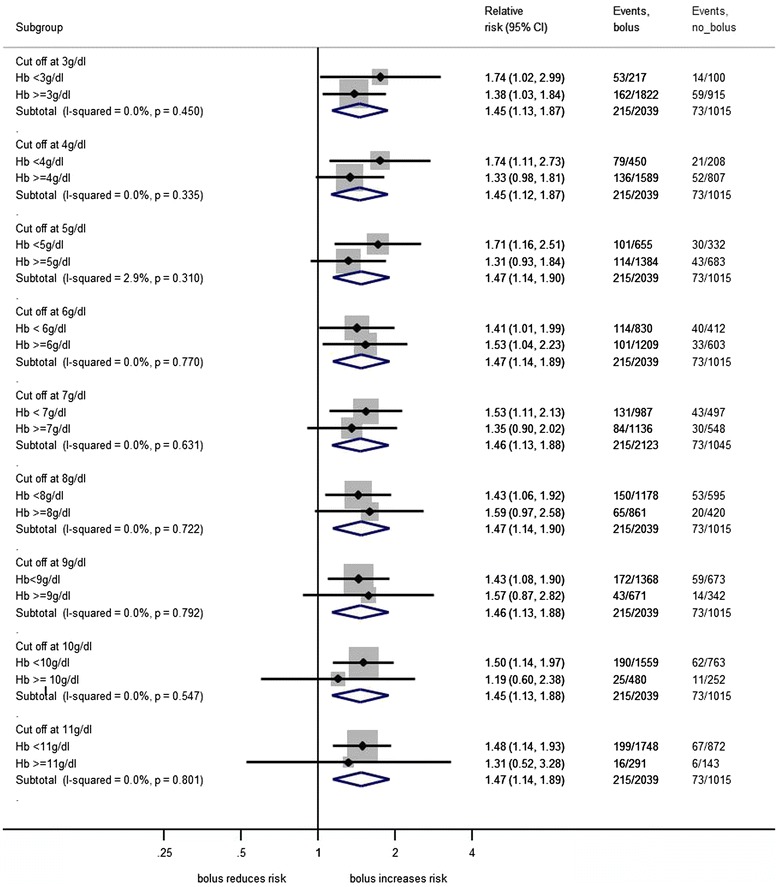
Of 3,170 children in the FEAST trial, 3,082 (97%) had baseline haemoglobin (Hb) measurement, 2,346/3,082 (76%) were anaemic (Hb <10 g/dL), and 33% severely anaemic (Hb <5 g/dL). Prevalence of severe anaemia varied from 12% in Kenya to 41% in eastern Uganda. 1,387/3,082 (45%) children were transfused (81% within 8 hours). Adherence to WHO transfusion guidelines was poor. Among severely anaemic children who were not transfused, 52% (54/103) died within 8 hours, and 90% of these deaths occurred within 2.5 hours of randomisation. By 24 hours, 128/1,002 (13%) severely anaemic children had died, compared to 36/501 (7%) and 71/843 (8%) of those with moderate and mild anaemia, respectively. Among children without severe hypotension who were randomised to receive fluid boluses of 0.9% saline or albumin, mortality was increased (10.6% and 10.5%, respectively) compared to controls (7.2%), regardless of admission Hb level. Repeat transfusion varied from ≤2% in Kenya/Tanzania to 6 to 13% at the four Ugandan centres. Adverse reactions to blood were rare (0.4%).
Severe anaemia complicates one third of childhood admissions with serious febrile illness to hospitals in East Africa, and is associated with increased mortality. A high proportion of deaths occurred within 2.5 hours of admission, emphasizing the need for rapid recognition and prompt blood transfusion. Adherence to current WHO transfusion guidelines was poor. The high rates of re-transfusion suggest that 20 mL/kg whole blood or 10 mL/kg packed cells may undertreat a significant proportion of anaemic children. Future evaluation of the impact of a larger volume of transfused blood and optimum transfusion management of children with Hb of <6 g/dL is warranted.
儿童严重贫血是撒哈拉以南非洲地区住院的主要原因及死亡的主要因素,但关于这一弱势群体输血情况的公开数据有限。
我们呈现了一项大型液体复苏对照试验(液体扩容作为支持性治疗(FEAST)试验)的数据,该试验针对在三个东非国家因严重发热性疾病(主要为疟疾和/或败血症)且外周灌注受损而住院的儿童贫血的患病率、临床特征及输血管理情况进行研究。
在FEAST试验的3170名儿童中,3082名(97%)进行了基线血红蛋白(Hb)测量,其中2346/3082名(76%)贫血(Hb<10g/dL),33%为严重贫血(Hb<5g/dL)。严重贫血的患病率从肯尼亚的12%到乌干达东部的41%不等。1387/3082名(45%)儿童接受了输血(81%在8小时内)。对世界卫生组织输血指南的依从性较差。在未输血的严重贫血儿童中,52%(54/103)在8小时内死亡,其中90%的死亡发生在随机分组后的2.5小时内。到24小时时,1002名严重贫血儿童中有128名(13%)死亡,中度贫血和轻度贫血儿童的这一比例分别为36/501(7%)和71/843(8%)。在未发生严重低血压且被随机分配接受0.9%生理盐水或白蛋白液体推注的儿童中,无论入院时Hb水平如何,与对照组(7.2%)相比,死亡率均有所增加(分别为10.6%和10.5%)。重复输血的比例在肯尼亚/坦桑尼亚为≤2%,在乌干达的四个中心为6%至13%。输血不良反应很少见(0.4%)。
严重贫血使东非地区三分之一因严重发热性疾病住院的儿童病情复杂化,并与死亡率增加相关联。很大一部分死亡发生在入院后的2.5小时内,这凸显了快速识别和及时输血的必要性。对当前世界卫生组织输血指南的依从性较差。再次输血率较高表明,20mL/kg全血或10mL/kg浓缩红细胞可能无法有效治疗相当一部分贫血儿童。有必要对输入更大血量以及对Hb<6g/dL儿童进行最佳输血管理的影响进行未来评估。