Akech Samuel O, Hassall Oliver, Pamba Allan, Idro Richard, Williams Thomas N, Newton Charles R J C, Maitland Kathryn
Centre for Geographic Medicine Research (Coast), Kenya Medical Research Institute, Kilifi, Kenya.
Malar J. 2008 Dec 16;7:256. doi: 10.1186/1475-2875-7-256.
Severe anaemia requiring emergency blood transfusion is a common complication of malaria in children. To ensure access for urgent blood transfusion, the World Health Organization has developed clear guidelines with haemoglobin thresholds prevent unwarranted transfusion,. Few studies have reported outcome and haematological recovery of children with severe malaria where transfusion practice complies with WHO recommendations.
A prospective observational study of survivors of severe and complicated malaria transfused in accordance with WHO guidelines. Children were invited for review at one month post-discharge. Non-attendees were traced in the community to ascertain survival.
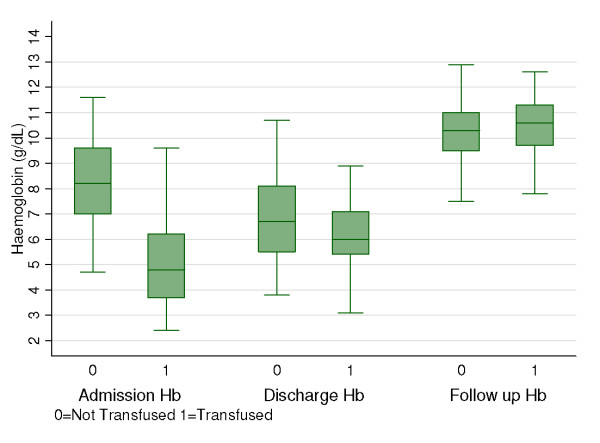
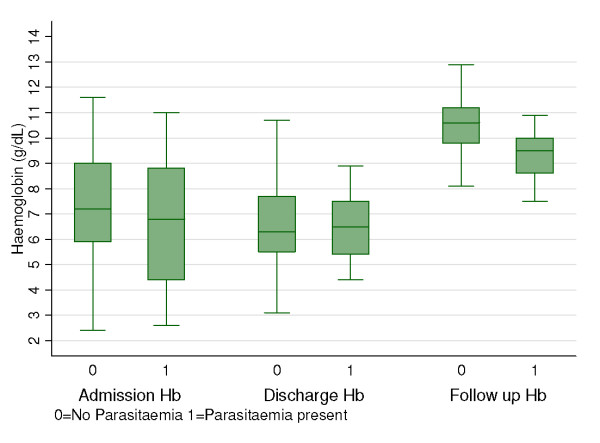
Outcome was assessed in 213 survivors. Those transfused were younger, had a higher base deficit, mean lactate levels and a higher prevalence of respiratory distress. As expected mean admission haemoglobin (Hb) was significantly lower amongst transfused [5.0 g/dL SD: 1.9] compared to non-transfused children [8.3 g/dL SD: 1.7] (p < 0.001). At discharge mean Hb was similar 6.4 g/dL [SD: 1.5] and 6.8 g/dL [SD: 1.6] respectively (p = 0.08), most children remained moderately to severely anaemic. At one month follow up 166 children (78%) returned, in whom we found no differences in mean Hb between the transfused (10.2 g/dL [SD: 1.7]) and non-transfused (10.0 g/dL [SD: 1.3]) survivors (p = 0.25). The major factors affecting haematological recovery were young age (<24 months) and concomitant malaria parasitaemia; Hb being 8.8 g/dL [SD: 1.5] in parasitaemic individuals compared with 10.5 g/dL [SD: 1.3] in those without (p < 0.001).
This data supports the policy of rational use of blood transfusion, as proposed in the WHO guidelines, for children with anaemia in areas where access to emergency transfusion is not guaranteed. We have provided empirical data indicating that transfusion does not influence superior recovery in haemoglobin concentrations and therefore cannot be justified on this basis alone. This may help resolve the disparity between international policy and current clinical practice. Effective anti-malarial treatment at discharge may prevent reoccurrence of anaemia.
需要紧急输血的严重贫血是儿童疟疾的常见并发症。为确保紧急输血的可及性,世界卫生组织制定了明确的指南,设定了血红蛋白阈值以防止不必要的输血。很少有研究报告严重疟疾患儿在输血实践符合世界卫生组织建议的情况下的治疗结果和血液学恢复情况。
对按照世界卫生组织指南输血的严重和复杂疟疾幸存者进行前瞻性观察研究。患儿在出院后1个月被邀请进行复查。未参加者在社区进行追踪以确定生存情况。
对213名幸存者的治疗结果进行了评估。接受输血的患儿年龄更小,碱缺失、平均乳酸水平更高,呼吸窘迫的患病率更高。正如预期的那样,接受输血的患儿入院时平均血红蛋白(Hb)水平[5.0 g/dL,标准差:1.9]显著低于未输血患儿[8.3 g/dL,标准差:1.7](p<0.001)。出院时平均Hb水平相似,分别为6.4 g/dL[标准差:1.5]和6.8 g/dL[标准差:1.6](p=0.08),大多数患儿仍为中度至重度贫血。在1个月的随访中,166名患儿(78%)返回,我们发现接受输血的幸存者(10.2 g/dL[标准差:1.7])和未输血的幸存者(10.0 g/dL[标准差:1.3])之间平均Hb水平无差异(p=0.25)。影响血液学恢复的主要因素是年龄小(<24个月)和合并疟疾寄生虫血症;有寄生虫血症的个体Hb为8.8 g/dL[标准差:1.5],而无寄生虫血症的个体为10.5 g/dL[标准差:1.3](p<0.001)。
这些数据支持世界卫生组织指南中提出的合理使用输血的政策,适用于无法保证紧急输血可及性地区的贫血患儿。我们提供的经验数据表明,输血不会影响血红蛋白浓度的更好恢复,因此不能仅基于此证明其合理性。这可能有助于解决国际政策与当前临床实践之间的差异。出院时有效的抗疟治疗可能预防贫血复发。