Eriksen Anne, Tillin Therese, O'Connor Laura, Brage Soren, Hughes Alun, Mayet Jamil, McKeigue Paul, Whincup Peter, Chaturvedi Nish, Forouhi Nita G
Medical Research Council Epidemiology Unit, University of Cambridge School of Clinical Medicine, Institute of Metabolic Science, Cambridge Biomedical Campus, Cambridge, United Kingdom.
University College London Institute of Cardiovascular Science, University College London, London, United Kingdom.
PLoS One. 2015 Mar 2;10(3):e0117364. doi: 10.1371/journal.pone.0117364. eCollection 2015.
There is consistent evidence on the impact of health behaviours on risk of cardiovascular disease (CVD) in European populations. As South Asians in the UK have an excess risk of CVD and coronary heart disease (CHD) compared to Europeans, we investigated whether a similar association between combined health behaviours and risk of CVD and CHD among this high-risk group exists, and estimated the population impact.
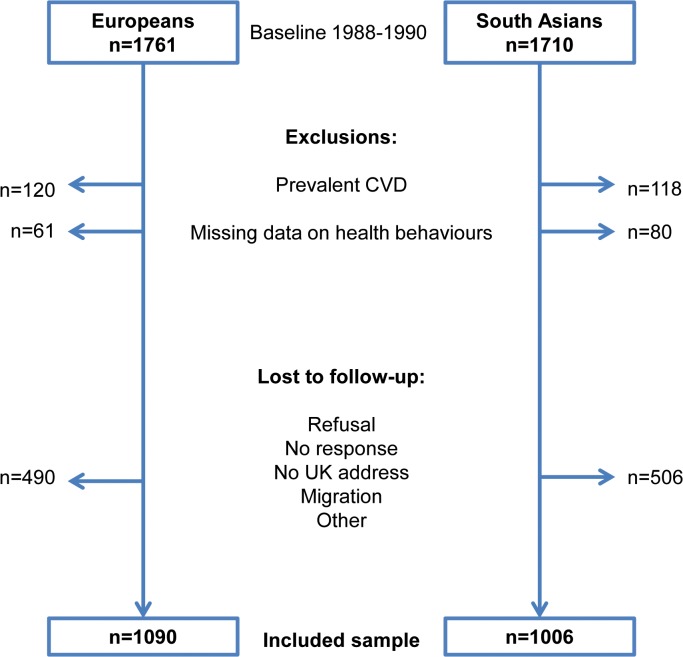
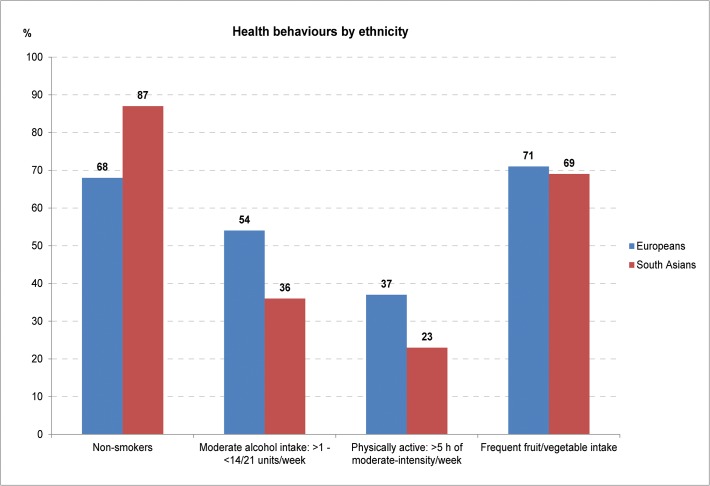
In a prospective cohort of 1090 Europeans and 1006 South Asians (40-69 y) without prevalent CVD at baseline (1988-1990), followed up for 21 years to 2011, there were 601 incident CVD events [Europeans n = 255; South Asians n = 346] of which 520 were CHD events [n = 207 and 313 respectively]. Participants scored between 0 to 4 points for a composite score including four baseline healthy behaviours (non-smoker, moderate alcohol intake, physically active, frequent fruit/vegetable intake). Adjusted hazard ratios (95% confidence intervals) for incident CHD in Europeans who had three, two, one, and zero compared to four health behaviours were 1.33 (0.78-2.29), 1.96 (1.15-3.33), 1.36 (0.74-2.48) and 2.45 (1.18-5.10), respectively, p-trend = 0.025. In South Asians, corresponding HRs were 2.88 (1.33-6.24), 2.28 (1.06-4.91), 3.36 (1.53-7.39) and 3.48 (1.38-8.81), p-trend = 0.022. The results were similar for incident CVD; Europeans HR 2.12 (1.14-3.94), p-trend = 0.014; South Asians HR 2.73 (1.20-6.21), p-trend = 0.018. The population attributable fraction in Europeans was 43% for CHD and 28% for CVD. In South Asians it was 63% and 51% respectively.
Lack of adherence to four combined health behaviours was associated with 2 to 3-fold increased risk of incident CVD in Europeans and South Asians. A substantial population impact in the South Asian group indicates important potential for disease prevention in this high-risk group by adherence to healthy behaviours.
关于健康行为对欧洲人群心血管疾病(CVD)风险的影响,已有一致的证据。由于与欧洲人相比,英国的南亚人患心血管疾病和冠心病(CHD)的风险更高,我们调查了这一高危人群中综合健康行为与心血管疾病和冠心病风险之间是否存在类似关联,并估计了对人群的影响。
在一个前瞻性队列中,有1090名欧洲人和1006名南亚人(40 - 69岁),基线时(1988 - 1990年)无心血管疾病,随访至2011年共21年,有601例心血管疾病事件发生[欧洲人n = 255;南亚人n = 346],其中520例为冠心病事件[分别为n = 207和313]。参与者在包括四项基线健康行为(不吸烟、适度饮酒、身体活跃、经常摄入水果/蔬菜)的综合评分中得分为0至4分。与具有四种健康行为的欧洲人相比,具有三种、两种、一种和零种健康行为的欧洲人发生冠心病的调整后风险比(95%置信区间)分别为1.33(0.78 - 2.29)、1.96(1.15 - 3.33)、1.36(0.74 - 2.48)和2.45(1.18 - 5.10),p趋势 = 0.025。在南亚人中,相应的风险比分别为2.88(1.33 - 6.24)、2.28(1.06 - 4.91)、3.36(1.53 - 7.39)和3.48(1.38 - 8.81),p趋势 = 0.022。心血管疾病事件的结果相似;欧洲人的风险比为2.12(1.14 - 3.94),p趋势 = 0.014;南亚人的风险比为2.73(1.20 - 6.21),p趋势 = 0.018。欧洲人群中冠心病的人群归因分数为43%,心血管疾病为28%。在南亚人中分别为63%和51%。
欧洲人和南亚人不遵守四种综合健康行为与心血管疾病发病风险增加2至3倍相关。南亚人群的大量人群影响表明,通过坚持健康行为,该高危人群在疾病预防方面具有重要潜力。