Mathukia Chirag, Fan WuQiang, Vadyak Karen, Biege Christine, Krishnamurthy Mahesh
Department of Medicine, Easton Hospital, Drexel University College of Medicine, Easton, PA, USA.
Department of Medicine, Easton Hospital, Drexel University College of Medicine, Easton, PA, USA;
J Community Hosp Intern Med Perspect. 2015 Apr 1;5(2):26716. doi: 10.3402/jchimp.v5.26716. eCollection 2015.
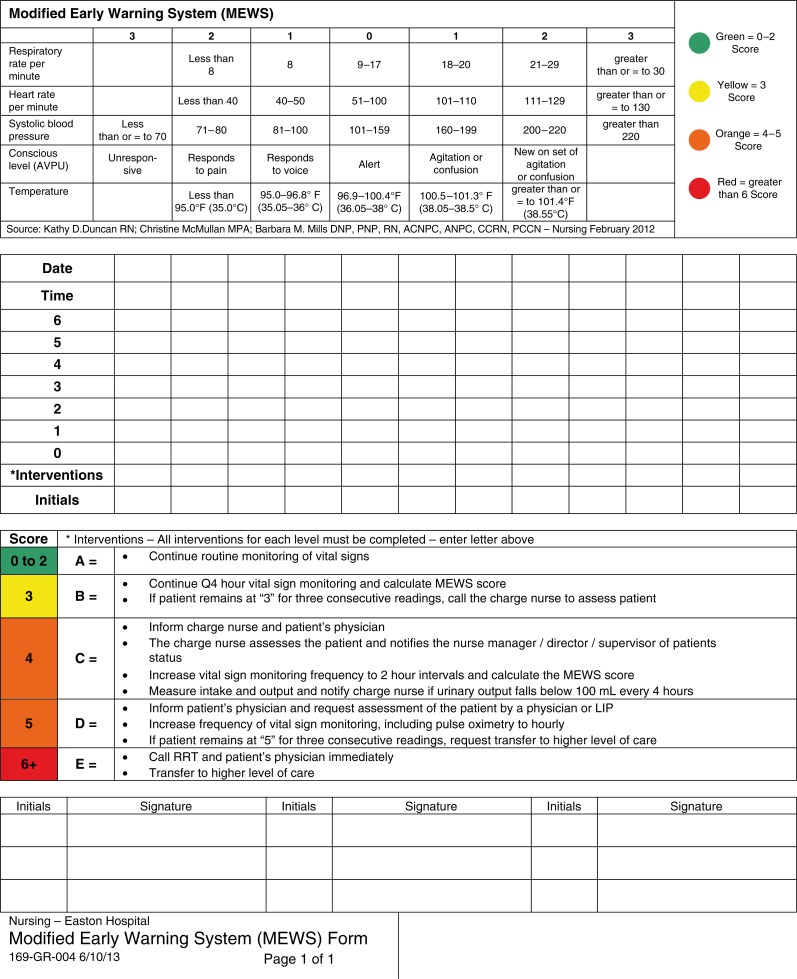
Severe adverse events such as cardiac arrest and death are often heralded by abnormal vital signs hours before the event. This necessitates an organized track and trigger approach of early recognition and response to subtle changes in a patient's condition. The Modified Early Warning System (MEWS) is one of such systems that use temperature, blood pressure, pulse, respiratory rate, and level of consciousness with each progressive higher score triggering an action. Root cause analysis for mortalities in our institute has led to the implementation of MEWS in an effort to improve patient outcomes. Here we discuss our experience and the impact of MEWS implementation on patient care at our community academic hospital.
MEWS was implemented in a protocolized manner in June 2013. The following data were collected from non-ICU wards on a monthly basis from January 2010 to June 2014: 1) number of rapid response teams (RRTs) per 100 patient-days (100PD); 2) number of cardiopulmonary arrests 'Code Blue' per 100PD; and 3) result of each RRT and Code Blue (RRT progressed to Code Blue, higher level of care, ICU transfer, etc.). Overall inpatient mortality data were also analyzed.
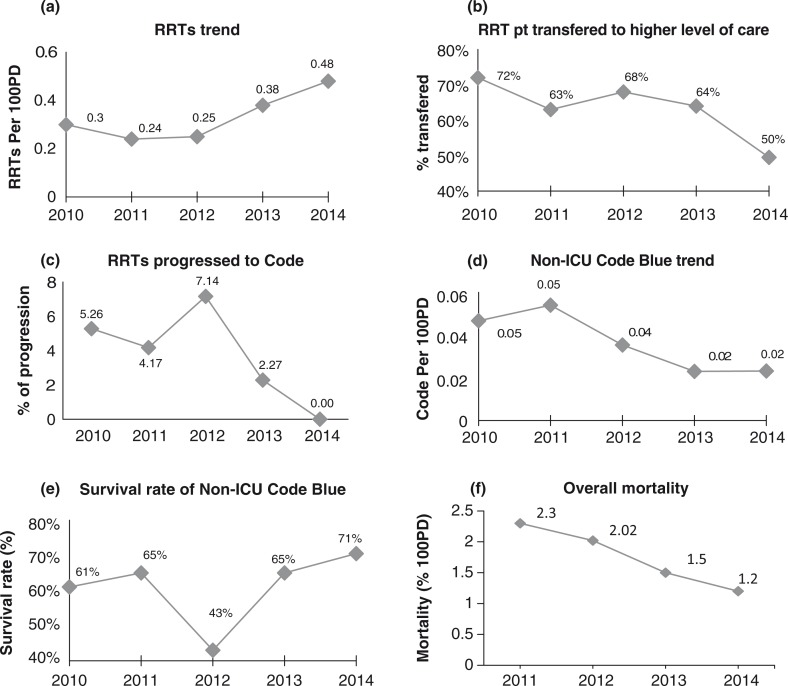
Since the implementation of MEWS, the number of RRT has increased from 0.24 per 100PD in 2011 to 0.38 per 100PD in 2013, and 0.48 per 100PD in 2014. The percentage of RRTs that progressed to Code Blue, an indicator of poor outcome of RRT, has been decreasing. In contrast, the numbers of Code Blue in non-ICU floors has been progressively decreasing from 0.05 per 100PD in 2011 to 0.02 per 100PD in 2013 and 2014. These improved clinical outcomes are associated with a decline of overall inpatient mortality rate from 2.3% in 2011 to 1.5% in 2013 and 1.2% in 2014.
Implementation of MEWS in our institute has led to higher rapid response system utilization but lower cardiopulmonary arrest events; this is associated with a lower mortality rate, and improved patient safety and clinical outcomes. We recommend the widespread use of MEWS to improve patient outcomes.
严重不良事件,如心脏骤停和死亡,往往在事件发生前数小时就会出现生命体征异常。这就需要一种有组织的跟踪和触发方法,以便早期识别并应对患者病情的细微变化。改良早期预警系统(MEWS)就是这样一种系统,它利用体温、血压、脉搏、呼吸频率和意识水平,每一个更高的分数都会触发相应行动。对我院死亡病例进行根本原因分析后,促使我们实施MEWS,以努力改善患者预后。在此,我们讨论我们的经验以及MEWS的实施对我们社区教学医院患者护理的影响。
2013年6月以标准化方式实施MEWS。从2010年1月至2014年6月,每月从非重症监护病房收集以下数据:1)每100患者日(100PD)的快速反应团队(RRT)数量;2)每100PD的心肺骤停“蓝色代码”数量;3)每个RRT和蓝色代码的结果(RRT进展为蓝色代码、更高水平护理、转入重症监护病房等)。还分析了总体住院患者死亡率数据。
自实施MEWS以来,RRT数量从2011年的每100PD 0.24增加到2013年的每100PD 0.38,2014年为每100PD 0.48。进展为蓝色代码的RRT百分比(RRT不良结局的一个指标)一直在下降。相比之下,非重症监护病房楼层的蓝色代码数量已从2011年的每100PD 0.05逐渐降至2013年和2014年的每100PD 0.02。这些改善的临床结局与总体住院患者死亡率从2011年的2.3%降至2013年的1.5%以及2014年的1.2%相关。
在我院实施MEWS导致快速反应系统利用率提高,但心肺骤停事件减少;这与较低的死亡率相关,并改善了患者安全和临床结局。我们建议广泛使用MEWS以改善患者预后。