Brenner Stephan, De Allegri Manuela, Gabrysch Sabine, Chinkhumba Jobiba, Sarker Malabika, Muula Adamson S
Institute of Public Health, Ruprecht-Karls-University, Heidelberg, Germany.
Department of Community Health, University of Malawi, College of Medicine, Blantyre, Malawi.
PLoS One. 2015 Apr 15;10(4):e0123968. doi: 10.1371/journal.pone.0123968. eCollection 2015.
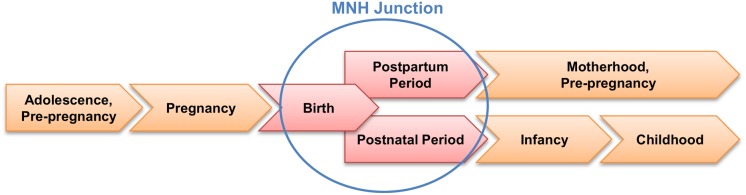
A variety of clinical process indicators exists to measure the quality of care provided by maternal and neonatal health (MNH) programs. To allow comparison across MNH programs in low- and middle-income countries (LMICs), a core set of essential process indicators is needed. Although such a core set is available for emergency obstetric care (EmOC), the 'EmOC signal functions', a similar approach is currently missing for MNH routine care evaluation. We describe a strategy for identifying core process indicators for routine care and illustrate their usefulness in a field example.
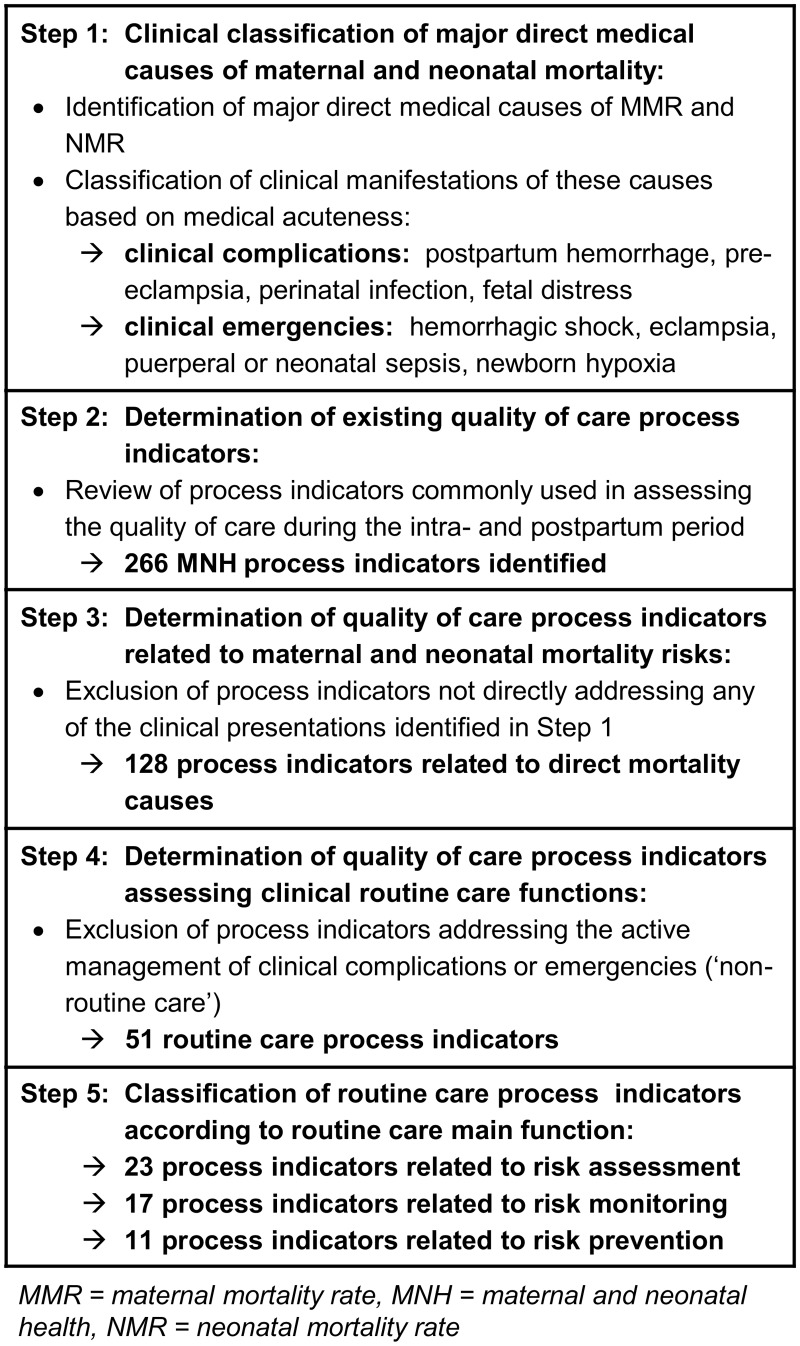
We first developed an indicator selection strategy by combining epidemiological and programmatic aspects relevant to MNH in LMICs. We then identified routine care process indicators meeting our selection criteria by reviewing existing quality of care assessment protocols. We grouped these indicators into three categories based on their main function in addressing risk factors of maternal or neonatal complications. We then tested this indicator set in a study assessing MNH quality of clinical care in 33 health facilities in Malawi.
Our strategy identified 51 routine care processes: 23 related to initial patient risk assessment, 17 to risk monitoring, 11 to risk prevention. During the clinical performance assessment a total of 82 cases were observed. Birth attendants' adherence to clinical standards was lowest in relation to risk monitoring processes. In relation to major complications, routine care processes addressing fetal and newborn distress were performed relatively consistently, but there were major gaps in the performance of routine care processes addressing bleeding, infection, and pre-eclampsia risks.
The identified set of process indicators could identify major gaps in the quality of obstetric and neonatal care provided during the intra- and immediate postpartum period. We hope our suggested indicators for essential routine care processes will contribute to streamlining MNH program evaluations in LMICs.
存在多种临床过程指标来衡量孕产妇和新生儿健康(MNH)项目所提供的护理质量。为了便于对低收入和中等收入国家(LMICs)的MNH项目进行比较,需要一套核心的基本过程指标。虽然急诊产科护理(EmOC)有这样一套核心指标,即“EmOC信号功能”,但目前在MNH常规护理评估中缺少类似的方法。我们描述了一种识别常规护理核心过程指标的策略,并通过一个实地案例说明其有用性。
我们首先通过结合与LMICs中MNH相关的流行病学和项目方面来制定指标选择策略。然后,通过审查现有的护理质量评估方案,确定符合我们选择标准的常规护理过程指标。我们根据这些指标在解决孕产妇或新生儿并发症风险因素方面的主要功能将其分为三类。然后,我们在一项评估马拉维33个卫生设施临床护理MNH质量的研究中测试了这套指标。
我们的策略确定了51个常规护理过程:23个与初始患者风险评估相关,17个与风险监测相关,11个与风险预防相关。在临床绩效评估中,共观察到82个案例。接生人员对临床标准的遵守在风险监测过程方面最低。关于主要并发症,处理胎儿和新生儿窘迫的常规护理过程执行相对一致,但在处理出血、感染和先兆子痫风险的常规护理过程执行方面存在重大差距。
所确定的过程指标集可以识别产时和产后即刻提供的产科和新生儿护理质量方面的主要差距。我们希望我们建议的基本常规护理过程指标将有助于简化LMICs中的MNH项目评估。