Takiar Radhika, Lutsey Pamela L, Zhao Di, Guallar Eliseo, Schneider Andrea L C, Grams Morgan E, Appel Lawrence J, Selvin Elizabeth, Michos Erin D
Northeast Ohio Medical University, Akron, OH, USA.
Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, MD, USA.
Bone. 2015 Sep;78:94-101. doi: 10.1016/j.bone.2015.04.029. Epub 2015 Apr 25.
Deficient levels of 25-hydroxyvitamin D [25(OH)D] have been associated with increased fracture risk. Racial differences in fracture risk may be related to differences in bioavailable vitamin D due to single nucleotide polymorphism (SNP) variations in the vitamin D binding protein (DBP).
We measured 25(OH)D levels in 12,781 middle-aged White and Black participants [mean age 57 years (SD 5.7), 25% Black] in the ARIC Study who attended the second examination from 1990-1992. Participants were genotyped for two DBP SNPs (rs4588 and rs7041). Incident hospitalized fractures were measured by abstracting hospital records for ICD-9 codes. We used Cox proportional hazards models to evaluate the association between 25(OH)D levels and risk of fracture with adjustment for possible confounders. Interactions were tested by race and DBP genotype.
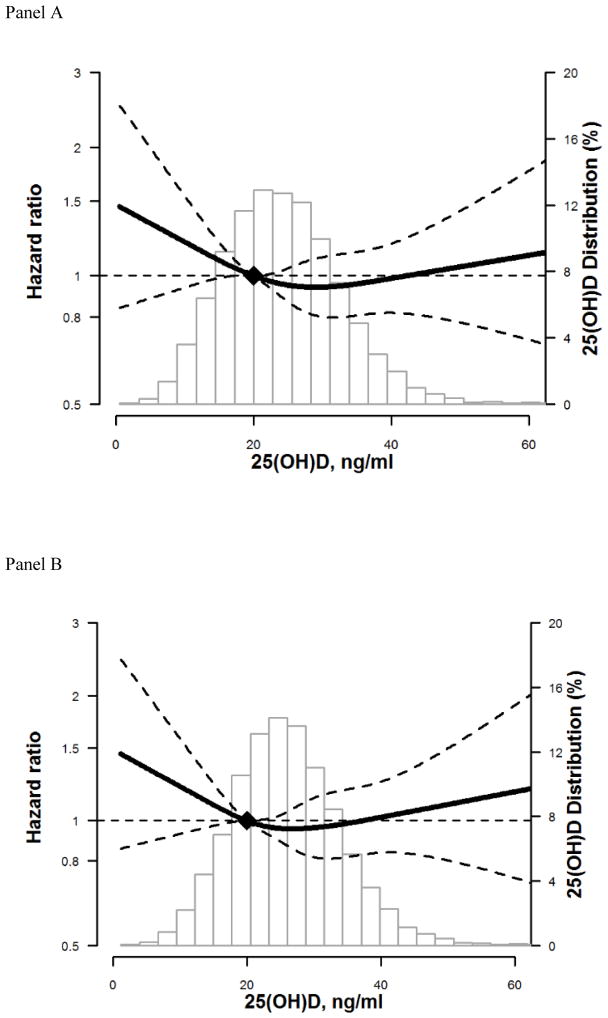
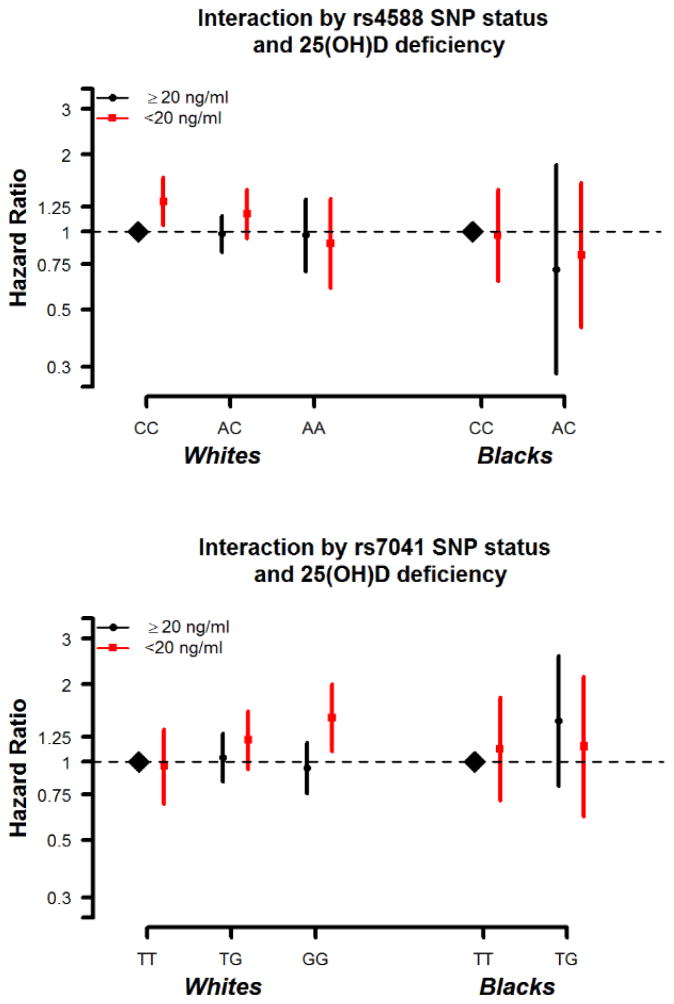
There were 1122 incident fracture-related hospitalizations including 267 hip fractures over a median of 19.6 years of follow-up. Participants with deficient 25(OH)D (<20 ng/mL) had a higher risk of any fracture hospitalization [HR=1.21 (95% CI 1.05-1.39)] and hospitalization for hip fracture [HR=1.35 (1.02-1.79)]. No significant racial interaction was noted (p-interaction=0.20 for any fracture; 0.74 for hip fracture). There was no independent association of rs4588 and rs7041 with fracture. However, there was a marginal interaction for 25(OH)D deficiency with rs7041 among Whites (p-interaction=0.065). Whites with both 25(OH)D deficiency and the GG genotype [i.e., with predicted higher levels of DBP and lower bioavailable vitamin D] were at the greatest risk for any fracture [HR=1.48 (1.10-2.00)] compared to Whites with the TT genotype and replete 25(OH)D (reference group).
Deficient 25(OH)D levels are associated with higher incidence of hospitalized fractures. Marginal effects were seen in Whites for the DBP genotype associated with lower bioavailable vitamin D, but result inconclusive. Further investigation is needed to more directly evaluate the association between bioavailable vitamin D and fracture risk.
25-羟基维生素D[25(OH)D]水平不足与骨折风险增加有关。骨折风险的种族差异可能与维生素D结合蛋白(DBP)的单核苷酸多态性(SNP)变异导致的生物可利用维生素D差异有关。
我们在ARIC研究中测量了12781名中年白人和黑人参与者[平均年龄57岁(标准差5.7),25%为黑人]的25(OH)D水平,这些参与者参加了1990 - 1992年的第二次检查。对参与者进行了两个DBP SNP(rs4588和rs7041)的基因分型。通过提取ICD - 9编码的医院记录来测量骨折相关的住院事件。我们使用Cox比例风险模型来评估25(OH)D水平与骨折风险之间的关联,并对可能的混杂因素进行调整。通过种族和DBP基因型来检验相互作用。
在中位随访19.6年期间,共有1122例与骨折相关的住院事件,其中包括267例髋部骨折。25(OH)D水平不足(<20 ng/mL)的参与者发生任何骨折住院的风险更高[风险比(HR)=1.21(95%置信区间1.05 - 1.39)],髋部骨折住院的风险更高[HR=1.35(1.02 - 1.79)]。未观察到显著的种族相互作用(任何骨折的p值交互作用=0.20;髋部骨折为0.74)。rs4588和rs7041与骨折无独立关联。然而,在白人中,25(OH)D缺乏与rs7041之间存在边缘性相互作用(p值交互作用=0.065)。与携带TT基因型且25(OH)D充足的白人(参照组)相比,同时存在25(OH)D缺乏和GG基因型[即预测DBP水平较高且生物可利用维生素D较低]的白人发生任何骨折的风险最高[HR=1.48(1.10 - 2.00)]。
25(OH)D水平不足与骨折住院发生率较高有关。在白人中观察到与生物可利用维生素D较低相关的DBP基因型存在边缘性影响,但结果尚无定论。需要进一步研究以更直接地评估生物可利用维生素D与骨折风险之间的关联。