Burgner David P, Cooper Matthew N, Moore Hannah C, Stanley Fiona J, Thompson Peter L, de Klerk Nicholas H, Carter Kim W
Murdoch Childrens Research Institute, Royal Children's Hospital, Parkville, Victoria, Australia; School of Paediatrics and Child Health, University of Western Australia, Crawley, Western Australia, Australia; Department of Paediatrics, University of Melbourne, Parkville, Victoria, Australia; Department of Paediatrics, Monash University, Clayton, Victoria, Australia.
Division of Population Sciences, Telethon Kids Institute, University of Western Australia, Subiaco, Western Australia, Australia.
PLoS One. 2015 May 4;10(5):e0125342. doi: 10.1371/journal.pone.0125342. eCollection 2015.
Pathogen-specific and overall infection burden may contribute to atherosclerosis and cardiovascular disease (CVD), but the effect of infection severity and timing is unknown. We investigated whether childhood infection-related hospitalisation (IRH, a marker of severity) was associated with subsequent adult CVD hospitalisation.
Using longitudinal population-based statutorily-collected administrative health data from Western Australia (1970-2009), we identified adults hospitalised with CVD (ischaemic heart disease, ischaemic stroke, and peripheral vascular disease) and matched them (10:1) to population controls. We used Cox regression to assess relationships between number and type of childhood IRH and adulthood CVD hospitalisation, adjusting for sex, age, Indigenous status, socioeconomic status, and birth weight.
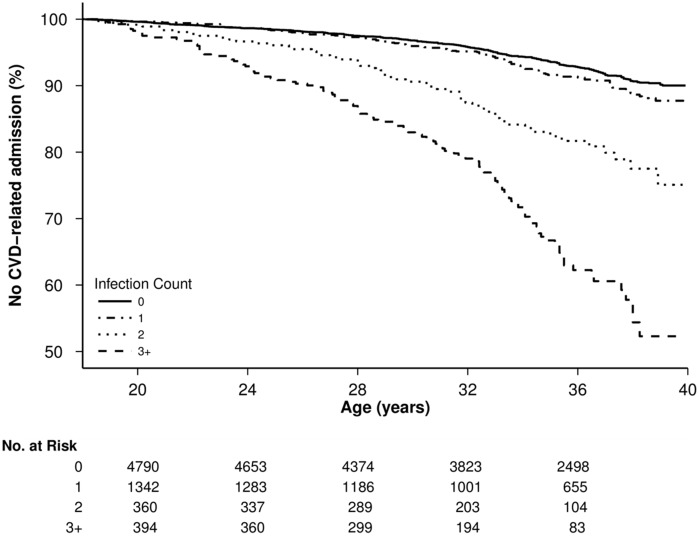
631 subjects with CVD-related hospitalisation in adulthood (≥ 18 years) were matched with 6310 controls. One or more childhood (< 18 years) IRH was predictive of adult CVD-related hospitalisation (adjusted hazard ratio, 1.3; 95% CI 1.1-1.6; P < 0.001). The association showed a dose-response; ≥ 3 childhood IRH was associated with a 2.2 times increased risk of CVD-related hospitalisation in adulthood (adjusted hazard ratio, 2.2; 95% CI 1.7-2.9; P < 0.001). The association was observed across all clinical diagnostic groups of infection (upper respiratory tract infection, lower respiratory tract infection, infectious gastroenteritis, urinary tract infection, skin and soft tissue infection, and other viral infection), and individually with CVD diagnostic categories (ischaemic heart disease, ischaemic stroke and peripheral vascular disease).
Severe childhood infection is associated with CVD hospitalisations in adulthood in a dose-dependent manner, independent of population-level risk factors.
病原体特异性感染负担和总体感染负担可能会导致动脉粥样硬化和心血管疾病(CVD),但感染严重程度和时机的影响尚不清楚。我们调查了儿童期与感染相关的住院治疗(IRH,一种严重程度的标志物)是否与随后的成人CVD住院治疗有关。
利用基于西澳大利亚州纵向人口的法定收集行政健康数据(1970 - 2009年),我们确定了因CVD(缺血性心脏病、缺血性中风和外周血管疾病)住院的成年人,并将他们与人群对照以10:1的比例进行匹配。我们使用Cox回归来评估儿童期IRH的数量和类型与成年期CVD住院治疗之间的关系,并对性别、年龄、原住民身份、社会经济地位和出生体重进行了调整。
631名成年期(≥18岁)因CVD相关住院的受试者与6310名对照进行了匹配。一次或多次儿童期(<18岁)IRH可预测成人CVD相关住院治疗(调整后的风险比,1.3;95%置信区间1.1 - 1.6;P<0.001)。这种关联呈现剂量反应关系;≥3次儿童期IRH与成年期CVD相关住院风险增加2.2倍相关(调整后的风险比,2.2;95%置信区间1.7 - 2.9;P<0.001)。在所有感染临床诊断组(上呼吸道感染、下呼吸道感染、感染性肠胃炎、尿路感染、皮肤和软组织感染以及其他病毒感染)中均观察到这种关联,并且在CVD诊断类别(缺血性心脏病、缺血性中风和外周血管疾病)中单独观察到。
儿童期严重感染与成年期CVD住院治疗呈剂量依赖性相关,独立于人群水平的风险因素。