Santos Itamar Souza, Goulart Alessandra Carvalho, Brandão Rodrigo Martins, Santos Rafael Caire de Oliveira, Bittencourt Márcio Sommer, Sitnik Débora, Pereira Alexandre Costa, Pastore Carlos Alberto, Samesima Nelson, Lotufo Paulo Andrade, Bensenor Isabela Martins
Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, BR.
Hospital Universitário, Universidade de São Paulo, São Paulo, SP, BR.
Arq Bras Cardiol. 2015 Jul;105(1):53-64. doi: 10.5935/abc.20150044. Epub 2015 May 8.
Information about post-acute coronary syndrome (ACS) survival have been mostly short-term findings or based on specialized, cardiology referral centers.
To describe one-year case-fatality rates in the Strategy of Registry of Acute Coronary Syndrome (ERICO) cohort, and to study baseline characteristics as predictors.
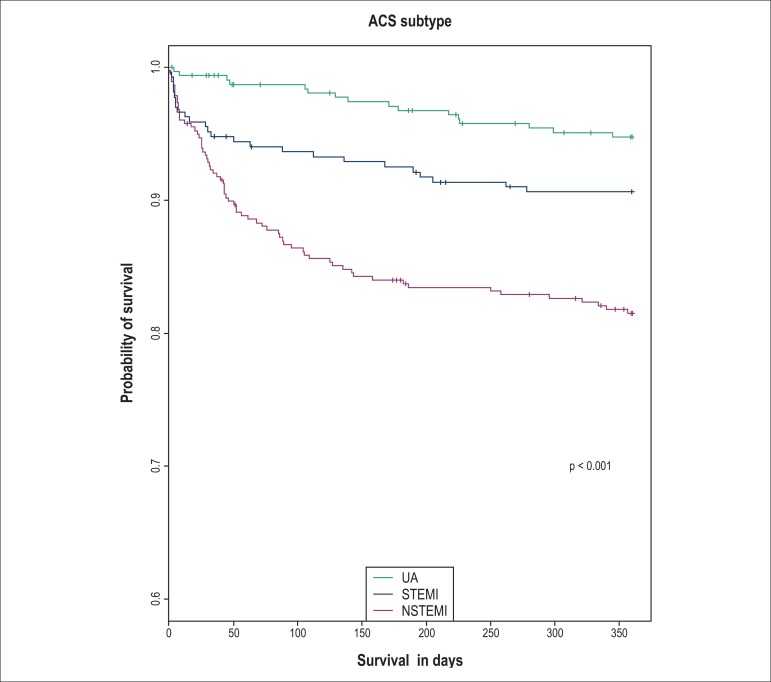
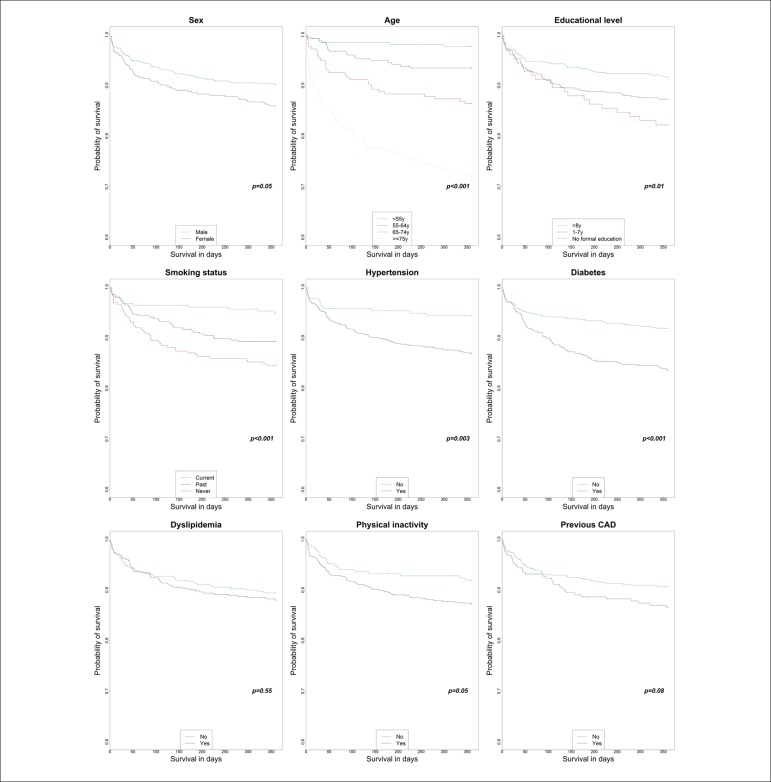
We analyzed data from 964 ERICO participants enrolled from February 2009 to December 2012. We assessed vital status by telephone contact and official death certificate searches. The cause of death was determined according to the official death certificates. We used log-rank tests to compare the probabilities of survival across subgroups. We built crude and adjusted (for age, sex and ACS subtype) Cox regression models to study if the ACS subtype or baseline characteristics were independent predictors of all-cause or cardiovascular mortality.
We identified 110 deaths in the cohort (case-fatality rate, 12.0%). Age [Hazard ratio (HR) = 2.04 per 10 year increase; 95% confidence interval (95%CI) = 1.75–2.38], non-ST elevation myocardial infarction (HR = 3.82 ; 95%CI = 2.21–6.60) or ST elevation myocardial infarction (HR = 2.59; 95%CI = 1.38–4.89) diagnoses, and diabetes (HR = 1.78; 95%CI = 1.20‑2.63) were significant risk factors for all-cause mortality in the adjusted models. We found similar results for cardiovascular mortality. A previous coronary artery disease diagnosis was also an independent predictor of all-cause mortality (HR = 1.61; 95%CI = 1.04–2.50), but not for cardiovascular mortality.
We found an overall one-year mortality rate of 12.0% in a sample of post-ACS patients in a community, non-specialized hospital in São Paulo, Brazil. Age, ACS subtype, and diabetes were independent predictors of poor one‑year survival for overall and cardiovascular-related causes.
关于急性冠状动脉综合征(ACS)后生存率的信息大多是短期研究结果,或基于专业的心脏病学转诊中心。
描述急性冠状动脉综合征登记策略(ERICO)队列中的一年病死率,并研究基线特征作为预测因素。
我们分析了2009年2月至2012年12月纳入的964名ERICO参与者的数据。通过电话联系和官方死亡证明搜索评估生命状态。根据官方死亡证明确定死亡原因。我们使用对数秩检验比较各亚组的生存概率。我们建立了粗模型和校正模型(校正年龄、性别和ACS亚型),以研究ACS亚型或基线特征是否是全因死亡或心血管死亡的独立预测因素。
我们在队列中确定了110例死亡(病死率为12.0%)。年龄[每增加10岁风险比(HR)=2.04;95%置信区间(95%CI)=1.75–2.38]、非ST段抬高型心肌梗死(HR = 3.82;95%CI = 2.21–6.60)或ST段抬高型心肌梗死(HR = 2.59;95%CI = 1.38–4.89)诊断以及糖尿病(HR = 1.78;95%CI = 1.20‑2.63)在校正模型中是全因死亡的显著危险因素。我们在心血管死亡方面发现了类似结果。既往冠状动脉疾病诊断也是全因死亡的独立预测因素(HR = 1.61;95%CI = 1.04–2.50),但不是心血管死亡的独立预测因素。
我们在巴西圣保罗一家社区非专科医院的ACS后患者样本中发现总体一年死亡率为12.0%。年龄、ACS亚型和糖尿病是总体及心血管相关原因导致一年生存率低的独立预测因素。