Jacobson Karen B, Moll Anthony P, Friedland Gerald H, Shenoi Sheela V
Icahn School of Medicine at Mount Sinai, New York, New York, United States of America.
Church of Scotland Hospital, Tugela Ferry, KwaZulu-Natal, South Africa.
PLoS One. 2015 May 19;10(5):e0127024. doi: 10.1371/journal.pone.0127024. eCollection 2015.
HIV and tuberculosis (TB) coinfection remains a major public health threat in sub-Saharan Africa. Integration and decentralization of HIV and TB treatment services are being implemented, but data on outcomes of this strategy are lacking in rural, resource-limited settings. We evaluated TB treatment outcomes in TB/HIV coinfected patients in an integrated and decentralized system in rural KwaZulu-Natal, South Africa.
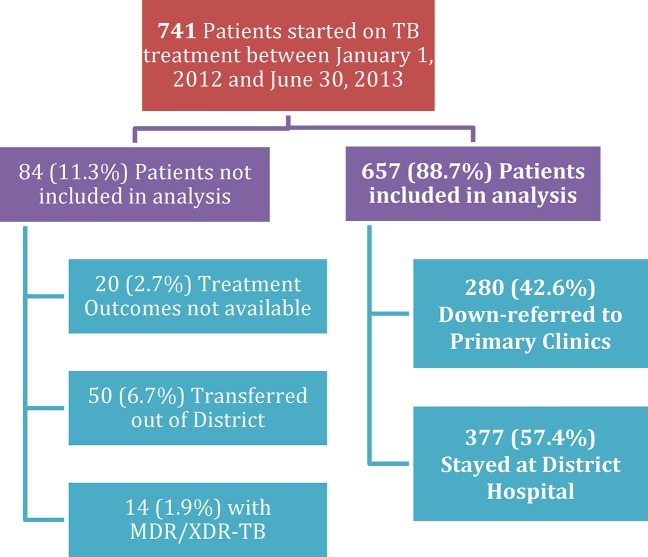
We retrospectively studied a cohort of HIV/TB coinfected patients initiating treatment for drug-susceptible TB at a district hospital HIV clinic from January 2012-June 2013. Patients were eligible for down-referral to primary health clinics(PHCs) for TB treatment completion if they met specific clinical criteria. Records were reviewed for patients' demographic, baseline clinical and laboratory information, past HIV and TB history, and TB treatment outcomes.
Of 657(88.7%) patients, 322(49.0%) were female, 558(84.9%) were new TB cases, and 572(87.1%) had pulmonary TB. After TB treatment initiation, 280(42.6%) were down-referred from the district level HIV clinic to PHCs for treatment completion; 377(57.4%) remained at the district hospital. Retained patients possessed characteristics indicative of more severe disease. In total, 540(82.2%) patients experienced treatment success, 69(10.5%) died, and 46(7.0%) defaulted. Down-referred patients experienced higher treatment success, and lower mortality, but were more likely to default, primarily at the time of transfer to PHC.
Decentralization of TB treatment to the primary care level is feasible in rural South Africa. Treatment outcomes are favorable when patients are carefully chosen for down-referral. Higher mortality in retained patients reflects increased baseline disease severity while higher default among down-referred patients reflects failed linkage of care. Better linkage mechanisms are needed including improved identification of potential defaulters, increased patient education, active communication between hospitals and PHCs, and tracing of patients lost to follow up. Decentralized and integrated care is successful for carefully selected TB/HIV coinfected patients and should be expanded.
在撒哈拉以南非洲地区,艾滋病毒(HIV)与结核病(TB)合并感染仍是一项重大的公共卫生威胁。HIV和TB治疗服务正在进行整合与去中心化,但在农村资源有限的环境中,缺乏关于该策略效果的数据。我们评估了南非夸祖鲁 - 纳塔尔省农村地区一个整合且去中心化系统中,HIV/TB合并感染患者的结核病治疗效果。
我们回顾性研究了一组于2012年1月至2013年6月在一家地区医院HIV诊所开始接受药物敏感型结核病治疗的HIV/TB合并感染患者队列。如果患者符合特定临床标准,就有资格被下转至基层医疗诊所(PHC)完成结核病治疗。对患者的人口统计学、基线临床和实验室信息、既往HIV和TB病史以及结核病治疗效果的记录进行了审查。
在657名(88.7%)患者中,322名(49.0%)为女性,558名(84.9%)为新发结核病病例,572名(87.1%)患有肺结核。开始结核病治疗后,280名(42.6%)患者从地区级HIV诊所被下转至PHC完成治疗;377名(57.4%)患者留在地区医院。留在医院的患者具有表明病情更严重的特征。总体而言,540名(82.2%)患者治疗成功,69名(10.5%)死亡,46名(7.0%)失访。下转患者的治疗成功率更高,死亡率更低,但更有可能失访,主要是在转至PHC时。
在南非农村地区,将结核病治疗去中心化至基层医疗层面是可行的。精心挑选下转的患者治疗效果良好。留在医院的患者死亡率较高反映了基线疾病严重程度增加,而下转患者中较高的失访率反映了医疗衔接失败。需要更好的衔接机制,包括改进对潜在失访者的识别、加强患者教育、医院与PHC之间的积极沟通以及对失访患者的追踪。对于精心挑选的HIV/TB合并感染患者,去中心化和整合式医疗是成功的,应予以推广。