Capogrosso Paolo, Boeri Luca, Ferrari Matteo, Ventimiglia Eugenio, La Croce Giovanni, Capitanio Umberto, Briganti Alberto, Damiano Rocco, Montorsi Francesco, Salonia Andrea
Division of Experimental Oncology, Unit of Urology, URI, IRCCS Ospedale San Raffaele, Milan; Research Doctorate Program in Urology, Magna Graecia University, Catanzaro, Italy.
Asian J Androl. 2016 Jan-Feb;18(1):85-9. doi: 10.4103/1008-682X.149180.
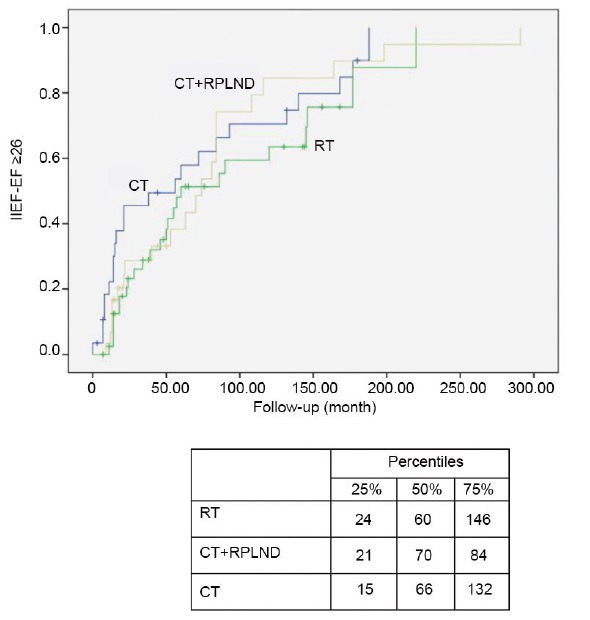
Testicular cancer (TC) is the most common solid cancer in men between the third and fourth decade of life. Due to successful treatment approaches, TC survivors (TCSs) have long life expectancy, but with numerous potential long-term sequelae, including sexual dysfunction. We investigated predictors of long-term normal sexual function (SF) recovery in TCSs. Sociodemographic, medical, and psychometric data were analyzed in 143 Caucasian-European TCSs, who underwent orchiectomy at a single institution. Health-significant comorbidities were scored with the Charlson Comorbidity Index (CCI). Patients completed the International Index of Erectile Function (IIEF). Statistical models tested the association between predictors (including age at surgery, body mass index, CCI, and adjuvant therapy: radiotherapy [RT], chemotherapy [CT], CT followed by retroperitoneal lymph node dissection [RPLND] and RPLND alone) and the long-term recovery of normal SF (defined as IIEF-erectile function [EF] ≥26, and sexual desire [SD], intercourse satisfaction [IS] orgasmic function [OF], and overall satisfaction [OS] domain scores in the upper tertiles). At a mean follow-up of 86 months, 35 (25.5%) TCSs had erectile dysfunction (ED), with 16 (11.2%) experiencing severe ED. Median time of EF recovery was 60, 60, and 70 months after CT, RT, and RPLND, respectively. Only adjuvant RT emerged as an independent predictor of nonrecovery of normal EF (HR: 0.55, P= 0.01). Neither adjuvant CT nor CT plus RPLND or RPLND alone significantly impaired the recovery of normal erections. Adjuvant therapy was not associated with impaired recovery of normal sexuality as a whole, considering the IIEF-SD, -OF, -IS, and OS domains.
睾丸癌(TC)是30至40岁男性中最常见的实体癌。由于治疗方法的成功,睾丸癌幸存者(TCSs)预期寿命较长,但存在许多潜在的长期后遗症,包括性功能障碍。我们调查了TCSs长期正常性功能(SF)恢复的预测因素。对143名在单一机构接受睾丸切除术的白种欧洲TCSs的社会人口统计学、医学和心理测量数据进行了分析。使用Charlson合并症指数(CCI)对具有健康意义的合并症进行评分。患者完成了国际勃起功能指数(IIEF)。统计模型测试了预测因素(包括手术年龄、体重指数、CCI和辅助治疗:放疗[RT]、化疗[CT]、CT后行腹膜后淋巴结清扫术[RPLND]和单独行RPLND)与正常SF长期恢复之间的关联(定义为IIEF勃起功能[EF]≥26,以及性欲[SD]、性交满意度[IS]、性高潮功能[OF]和总体满意度[OS]领域得分处于上三分位数)。在平均随访86个月时,35名(25.5%)TCSs存在勃起功能障碍(ED),其中16名(11.2%)为重度ED。CT、RT和RPLND后EF恢复的中位时间分别为60、60和70个月。只有辅助放疗是正常EF未恢复的独立预测因素(HR:0.55,P = 0.01)。辅助化疗、化疗加RPLND或单独行RPLND均未显著损害正常勃起功能的恢复。考虑到IIEF-SD、-OF、-IS和OS领域,辅助治疗与整体正常性功能恢复受损无关。