Vanmassenhove Jill, Lameire Norbert, Dhondt Annemieke, Vanholder Raymond, Van Biesen Wim
Renal Division, Ghent University Hospital, Nephrology section, 0 K12, University Hospital, De Pintelaan 185, B9000, Ghent, Belgium.
BMC Nephrol. 2015 Jul 22;16:112. doi: 10.1186/s12882-015-0107-4.
It is unclear how modifications in the way to calculate serum creatinine (sCr) increase and in the cut-off value applied, influences the prognostic value of Acute Kidney Injury (AKI). We wanted to evaluate whether these modifications alter the prognostic value of AKI for prediction of mortality at 3 months, 1 and 2 years.
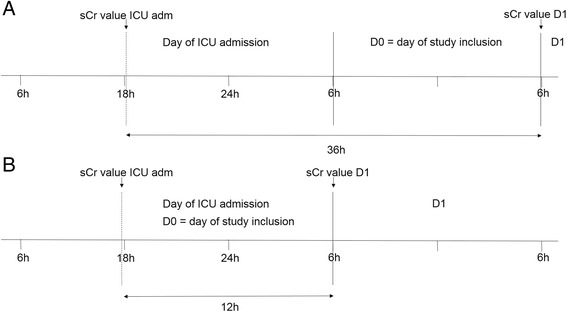
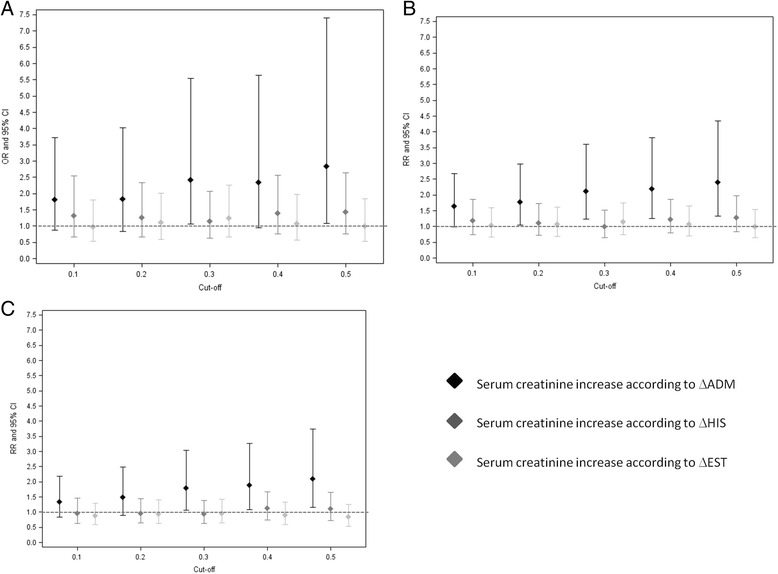
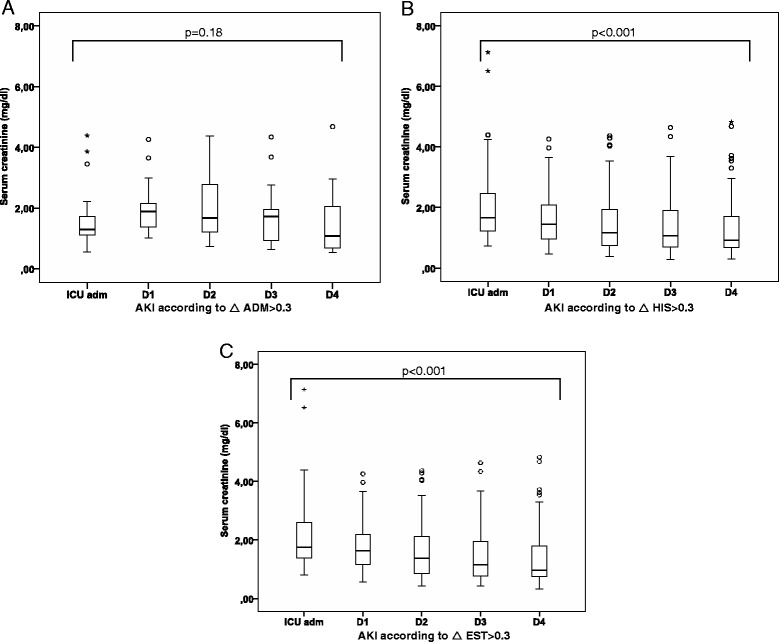
We prospectively included 195 septic patients and evaluated the prognostic value of AKI by using three different algorithms to calculate sCr increase: either as the difference between the highest value in the first 24 h after ICU admission and a pre-admission historical (ΔHIS) or an estimated (ΔEST) baseline value, or by subtracting the ICU admission value from the sCr value 24 h after ICU admission (ΔADM). Different cut-off levels of sCr increase (0.1, 0.2, 0.3, 0.4 and 0.5 mg/dl) were evaluated.
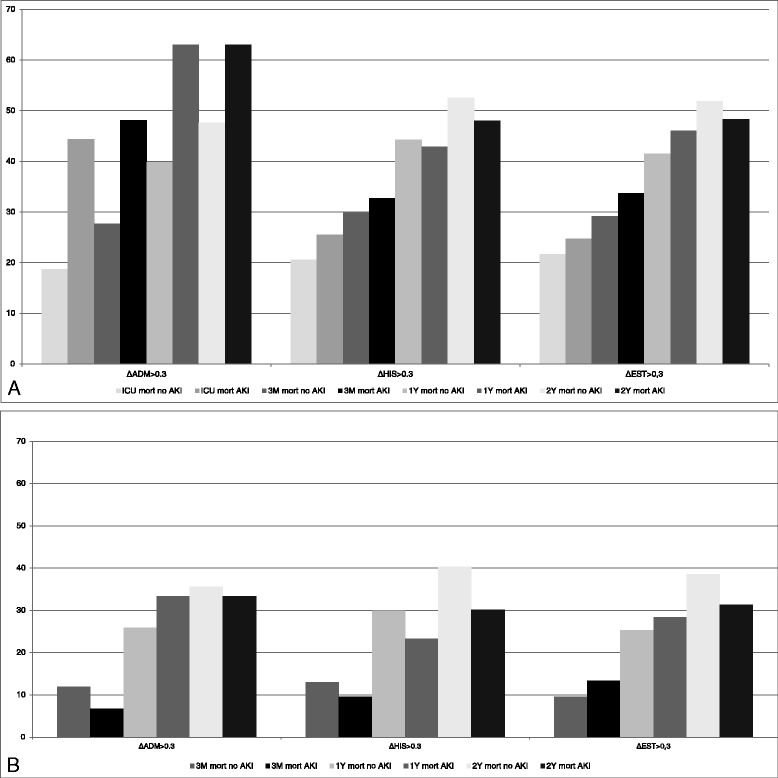
Mortality at 3 months, 1 and 2 years in AKI defined as ΔADM > 0.3 mg/dl was 48.1 %, 63.0 % and 63.0 % vs 27.7 %, 39.8 % and 47.6 % in no AKI respectively (OR(95%CI): 2.42(1.06-5.54), 2.58(1.11-5.97) and 1.87(0.81-4.33); 0.3 mg/dl was the lowest cut-off value that was discriminatory. When AKI was defined as ΔHIS > 0.3 mg/dl or ΔEST > 0.3 mg/dl, there was no significant difference in mortality between AKI and no AKI.
The prognostic value of a 0.3 mg/dl increase in sCr, on mortality in sepsis, depends on how this sCr increase is calculated. Only if the evolution of serum creatinine over the first 24 h after ICU admission is taken into account, an association with mortality is found.
目前尚不清楚血清肌酐(sCr)升高的计算方式及所应用的临界值的改变如何影响急性肾损伤(AKI)的预后价值。我们想评估这些改变是否会改变AKI对3个月、1年和2年死亡率预测的预后价值。
我们前瞻性纳入了195例脓毒症患者,并通过三种不同的算法计算sCr升高来评估AKI的预后价值:即重症监护病房(ICU)入院后最初24小时内的最高值与入院前历史(ΔHIS)或估计(ΔEST)基线值之间的差值,或者用ICU入院24小时后的sCr值减去ICU入院时的值(ΔADM)。评估了不同的sCr升高临界值水平(0.1、0.2、0.3、0.4和0.5mg/dl)。
定义为ΔADM>0.3mg/dl的AKI患者3个月、1年和2年的死亡率分别为48.1%、63.0%和63.0%,而无AKI患者分别为27.7%、39.8%和47.6%(比值比[95%置信区间]:2.42[1.06 - 5.54]、2.58[1.11 - 5.97]和1.87[0.81 - 4.33]);0.3mg/dl是具有鉴别意义的最低临界值。当AKI定义为ΔHIS>0.3mg/dl或ΔEST>0.3mg/dl时,AKI和无AKI患者的死亡率无显著差异。
sCr升高0.3mg/dl对脓毒症死亡率的预后价值取决于sCr升高的计算方式。只有考虑到ICU入院后最初24小时内血清肌酐的变化,才能发现其与死亡率的关联。