Bhatraju Pavan K, Mukherjee Paramita, Robinson-Cohen Cassianne, O'Keefe Grant E, Frank Angela J, Christie Jason D, Meyer Nuala J, Liu Kathleen D, Matthay Michael A, Calfee Carolyn S, Christiani David C, Himmelfarb Jonathan, Wurfel Mark M
Division of Pulmonary and Critical Care Medicine, University of Washington, Harborview Medical Center, 325 9th Avenue, Seattle, WA, 98104, USA.
Kidney Research Institute, University of Washington, Seattle, WA, USA.
Crit Care. 2016 Nov 17;20(1):372. doi: 10.1186/s13054-016-1546-4.
Acute kidney injury (AKI) is common among intensive care unit (ICU) patients. AKI is highly heterogeneous, with variable links to poor outcomes. Current approaches to classify AKI severity and identify patients at highest risk for poor outcomes focus on the maximum change in serum creatinine (SCr) values. However, these scores are hampered by the need for a reliable baseline SCr value and the absence of a component differentiating transient from persistent rises in SCr. We hypothesized that identification of resolving or nonresolving AKI subphenotypes based on the early trajectory of SCr values in the ICU would better differentiate patients at risk of hospital mortality.
We performed a secondary analysis of two prospective studies of ICU patients admitted to a trauma ICU (group 1; n = 1914) or general medical-surgical ICUs (group 2; n = 1867). In group 1, we tested definitions for resolving and nonresolving AKI subphenotypes and selected the definitions resulting in subphenotypes with the greatest separation in risk of death relative to non-AKI controls. We applied this definition to group 2 and tested whether the subphenotypes were independently associated with hospital mortality after adjustment for AKI severity.
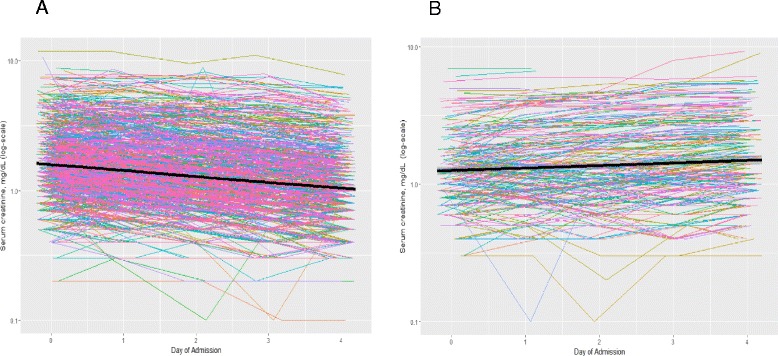
AKI occurred in 46% and 69% of patients in groups 1 and 2, respectively. In group 1, a resolving AKI subphenotype (defined as a decrease in SCr of 0.3 mg/dl or 25% from maximum in the first 72 h of study enrollment) was associated with a low risk of death. A nonresolving AKI subphenotype (defined as all AKI cases not meeting the "resolving" definition) was associated with a high risk of death. In group 2, the resolving AKI subphenotype was not associated with increased mortality (relative risk [RR] 0.86, 95% CI 0.63-1.17), whereas the nonresolving AKI subphenotype was associated with higher mortality (RR 1.68, 95% CI 1.15-2.44) even after adjustment for AKI severity stage.
The trajectory of SCr levels identifies AKI subphenotypes with different risks for death, even among AKI cases of similar severity. These AKI subphenotypes might better define the patients at risk for poor outcomes who might benefit from novel interventions.
急性肾损伤(AKI)在重症监护病房(ICU)患者中很常见。AKI具有高度异质性,与不良预后的关联各不相同。目前用于分类AKI严重程度和识别预后最差风险最高患者的方法侧重于血清肌酐(SCr)值的最大变化。然而,这些评分受到需要可靠的基线SCr值以及缺乏区分SCr短暂升高和持续升高的因素的限制。我们假设,根据ICU中SCr值的早期变化轨迹来识别AKI的缓解或未缓解亚表型,将能更好地区分有医院死亡风险的患者。
我们对两项前瞻性研究进行了二次分析,这两项研究涉及入住创伤ICU的患者(第1组;n = 1914)或普通内科-外科ICU的患者(第2组;n = 1867)。在第1组中,我们测试了AKI缓解和未缓解亚表型的定义,并选择了相对于非AKI对照组在死亡风险上有最大差异的亚表型定义。我们将此定义应用于第2组,并测试了在调整AKI严重程度后,这些亚表型是否与医院死亡率独立相关。
第1组和第2组中分别有46%和69%的患者发生AKI。在第1组中,一种AKI缓解亚表型(定义为在研究入组的前72小时内SCr从最高值下降0.3mg/dl或25%)与低死亡风险相关。一种AKI未缓解亚表型(定义为所有不符合“缓解”定义的AKI病例)与高死亡风险相关。在第2组中,AKI缓解亚表型与死亡率增加无关(相对风险[RR] 0.86,95%置信区间0.63 - 1.17),而AKI未缓解亚表型即使在调整AKI严重程度阶段后仍与较高死亡率相关(RR 1.68,95%置信区间1.15 - 2.44)。
SCr水平的变化轨迹可识别出具有不同死亡风险的AKI亚表型,即使在严重程度相似的AKI病例中也是如此。这些AKI亚表型可能能更好地界定那些可能从新干预措施中获益的预后不良风险患者。