Perrella Sharon L, Lai Ching T, Geddes Donna T
School of Chemistry and Biochemistry, M310, The University of Western Australia, 35 Stirling Highway, Crawley, WA, 6009, Australia.
BMC Pregnancy Childbirth. 2015 Jul 26;15:155. doi: 10.1186/s12884-015-0593-1.
Nipple pain is associated with early cessation of breastfeeding and may be caused by high intra-oral vacuum. However identification of high intra-oral vacuum is typically restricted to the research setting. This is the first reported case of an infant with high intra-oral vacuum that was clinically identified through a specific pattern of nipple trauma associated with nipple shield use. Knowledge of clinical signs associated with high intra-oral vacuum may facilitate early recognition of this unusual breastfeeding challenge.
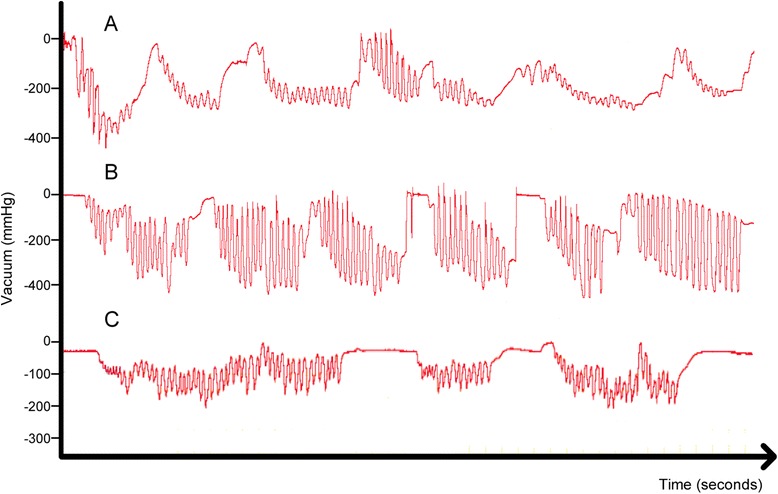
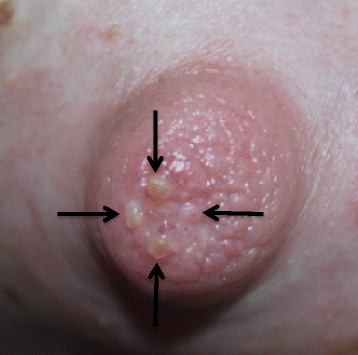
The mother of an exclusively breastfed 3 month old infant had severe bilateral nipple pain with minimal trauma that persisted from birth. The nipples were not misshapen immediately after breastfeeding and adjustments to infant attachment at the breast did not attenuate the pain. Examination of the infant's oral anatomy was unremarkable with no ankyloglossia present. Microbiological cultures of nipple swabs and breast milk were negative for bacterial and fungal growth, and prescribed antimicrobial treatments did not reduce the nipple pain. Mild blanching and erythema of the nipples were occasionally observed, and were not consistent with nipple vasospasm. Nipple shields were used regularly as they modified the pain, although this resulted in blisters that corresponded with the nipple shield holes. Measurement of infant intra-oral vacuum during breastfeeding confirmed intra-oral vacuum up to 307 % higher than reference values. Breastfeeding gradually became less painful, and after 6 months was completely comfortable.
High intra-oral vacuum is difficult to assess in the clinical setting and is likely an under-reported cause of early weaning that is not well understood. This original case report highlights high intra-oral vacuum as at differential diagnosis to be considered by health professionals when evaluating mothers experiencing strong nipple pain during the initiation of breastfeeding. A clinical screening tool is needed to enable prompt identification of these infants.
乳头疼痛与母乳喂养早期停止有关,可能由口腔内高负压引起。然而,口腔内高负压的识别通常仅限于研究环境。这是首例通过与乳头保护罩使用相关的特定乳头损伤模式在临床上识别出高口腔内负压的婴儿病例。了解与高口腔内负压相关的临床体征可能有助于早期识别这一不寻常的母乳喂养挑战。
一名纯母乳喂养3个月大婴儿的母亲双侧乳头剧痛,仅有轻微创伤,自婴儿出生后疼痛一直持续。母乳喂养后乳头没有立即变形,调整婴儿在乳房上的含接方式也未能减轻疼痛。检查婴儿口腔解剖结构未见异常,无舌系带过短。乳头拭子和母乳的微生物培养结果显示细菌和真菌生长均为阴性,所开的抗菌治疗并未减轻乳头疼痛。偶尔观察到乳头有轻度苍白和红斑,但不符合乳头血管痉挛的表现。尽管使用乳头保护罩会导致与保护罩孔相对应的水泡,但由于能缓解疼痛,仍经常使用。母乳喂养期间测量婴儿口腔内负压证实,其口腔内负压比参考值高出307%。母乳喂养的疼痛逐渐减轻,6个月后完全无痛。
在临床环境中难以评估口腔内高负压,它可能是早期断奶的一个未被充分报道且未被充分理解的原因。这例原始病例报告强调,在评估母乳喂养开始时经历强烈乳头疼痛的母亲时,健康专业人员应将高口腔内负压作为一个需要考虑的鉴别诊断因素。需要一种临床筛查工具来及时识别这些婴儿。