Saito Takahiro, Makino Takashi, Hata Yoshinobu, Koezuka Satoshi, Otsuka Hajime, Isobe Kazutoshi, Tochigi Naobumi, Shibuya Kazutoshi, Homma Sakae, Iyoda Akira
Division of Chest Surgery, Toho University School of Medicine, Tokyo, Japan.
Division of Respiratory Medicine, Toho University School of Medicine, Tokyo, Japan.
J Cardiothorac Surg. 2015 Sep 1;10:110. doi: 10.1186/s13019-015-0321-y.
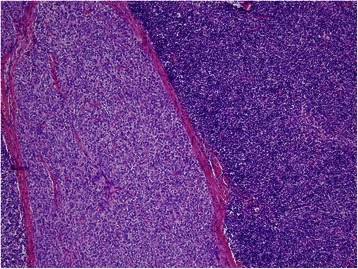
The appropriate surgical approach for a large mediastinal tumor is controversial. Median sternotomy is the standard approach for thymomas. We herein report the case of a giant thymoma, 13 cm in diameter, surgically resected via anterolateral incision. Subsequent thymectomy was performed via thoracoscopy. The resected specimen was a WHO type AB thymoma, Masaoka stage I, without capsular invasion. The anterolateral incision was less invasive and more versatile in the present case, as the incision could be extended to a hemiclamshell or posterolateral incision depending on exposure and relationship to adjacent organs and vascular structures.
对于大型纵隔肿瘤,合适的手术入路存在争议。正中胸骨切开术是胸腺瘤的标准手术入路。我们在此报告一例直径13厘米的巨大胸腺瘤病例,通过前外侧切口进行手术切除。随后通过胸腔镜进行胸腺切除术。切除标本为世界卫生组织AB型胸腺瘤,马萨oka分期I期,无包膜侵犯。在前外侧切口在本病例中侵袭性较小且更具通用性,因为根据暴露情况以及与相邻器官和血管结构的关系,该切口可扩展为半蛤壳式或后外侧切口。