Singh Shivinder, Goyal Rakhee, Upadhyay Kishan Kumar, Sethi Navdeep, Sharma Ram Murti, Sharma Anoop
Department of Anaesthesiology, Armed Forces Medial College, Pune, Maharashtra, India.
J Anaesthesiol Clin Pharmacol. 2015 Jul-Sep;31(3):370-4. doi: 10.4103/0970-9185.161675.
This study was carried out to evaluate the difference in efficacy, safety, and complications of performing brachial plexus nerve blocks by using a nerve locator when compared to ultrasound (US) guidance.
A total of 102 patients undergoing upper limb surgery under supraclavicular brachial plexus blocks were randomly divided into two groups, one with US and the other with nerve stimulator (NS). In Group US, "Titan" Portable US Machine, Sonosite, Inc. Kensington, UK with a 9.0 MHz probe was used to visualize the brachial plexus and 40 ml of 0.25% bupivacaine solution was deposited around the brachial plexus in a graded manner. In Group (NS), the needle was inserted 1-1.5 cm above mid-point of clavicle. Once hand or wrist motion was detected at a current intensity of less than 0.4 mA 40 ml of 0.25% bupivacaine was administered. Onset of sensory and motor block of radial, ulnar and median nerves was recorded at 5-min intervals for 30-min. Block execution time, duration of block (time to first analgesic), inadvertent vascular puncture, and neurological complications were taken as the secondary outcome variables.
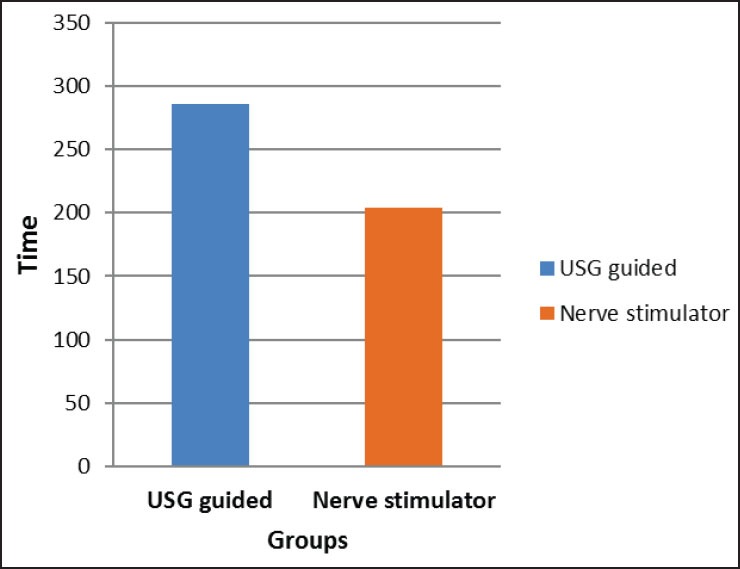
About 90% patients in US group and 73.1% in NS group, had successful blocks P = 0.028. The onset of block was faster in the Group US as compared to Group NS and this difference was significant (P 0.007) only in the radial nerve territory. The mean duration of the block was longer in Group US, 286.22 ± 42.339 compared to 204.37 ± 28.54-min in Group NS (P < 0.05). Accidental vascular punctures occurred in 7 patients in the NS group and only 1 patient in the US group.
Ultrasound guidance for supraclavicular brachial plexus blockade provides a block that is faster in onset, has a better quality and lasts longer when compared with an equal dose delivered by conventional means.
本研究旨在评估与超声(US)引导相比,使用神经定位仪进行臂丛神经阻滞在疗效、安全性及并发症方面的差异。
总共102例接受锁骨上臂丛阻滞下上肢手术的患者被随机分为两组,一组采用超声引导,另一组采用神经刺激器(NS)引导。在超声引导组(US组),使用英国肯辛顿索诺声公司的“泰坦”便携式超声仪及9.0MHz探头来可视化臂丛神经,并将40ml 0.25%布比卡因溶液分次注射于臂丛神经周围。在神经刺激器引导组(NS组),将穿刺针插入锁骨中点上方1 - 1.5cm处。一旦在电流强度小于0.4mA时检测到手或腕部运动,即给予40ml 0.25%布比卡因。每隔5分钟记录桡神经、尺神经和正中神经感觉及运动阻滞的起效情况,持续记录30分钟。阻滞执行时间、阻滞持续时间(至首次镇痛的时间)、意外血管穿刺及神经并发症被作为次要观察变量。
超声引导组约90%的患者阻滞成功,神经刺激器引导组为73.1%,P = 0.028。与神经刺激器引导组相比,超声引导组的阻滞起效更快,且仅在桡神经区域该差异具有统计学意义(P < 0.007)。超声引导组的平均阻滞持续时间更长,为286.22 ± 42.339分钟,而神经刺激器引导组为204.37 ± 28.54分钟(P < 0.05)。神经刺激器引导组有7例患者发生意外血管穿刺,超声引导组仅有1例。
与传统方法给予相同剂量药物相比,超声引导下锁骨上臂丛阻滞起效更快、质量更好且持续时间更长。