Schmid Patrick, Bregenzer Andrea, Huber Milo, Rauch Andri, Jochum Wolfram, Müllhaupt Beat, Vernazza Pietro, Opravil Milos, Weber Rainer
Division of Infectious Diseases and Hospital Epidemiology, Cantonal Hospital St. Gallen, St. Gallen, Switzerland.
Division of Infectious Diseases and Hospital Epidemiology, University Hospital Zurich, University of Zurich, Zurich, Switzerland.
PLoS One. 2015 Sep 29;10(9):e0138838. doi: 10.1371/journal.pone.0138838. eCollection 2015.
To evaluate the diagnostic performance of seven non-invasive tests (NITs) of liver fibrosis and to assess fibrosis progression over time in HIV/HCV co-infected patients.
Transient elastography (TE) and six blood tests were compared to histopathological fibrosis stage (METAVIR). Participants were followed over three years with NITs at yearly intervals.
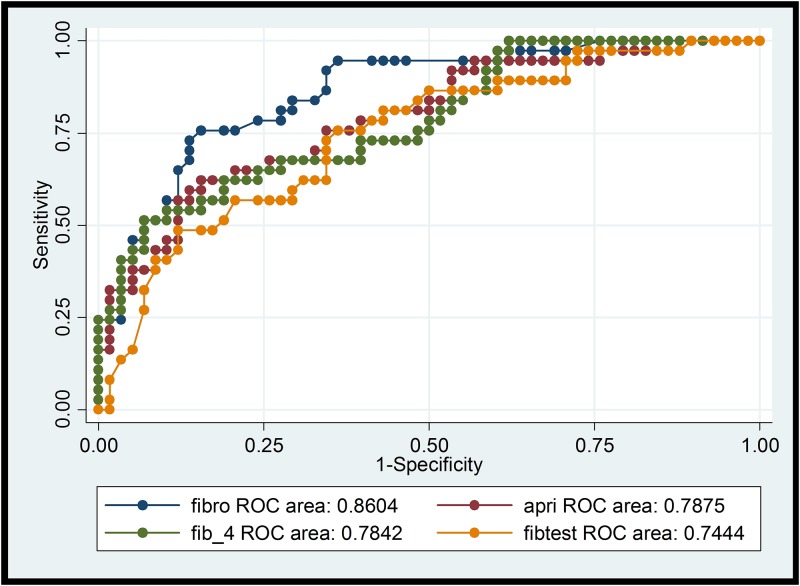
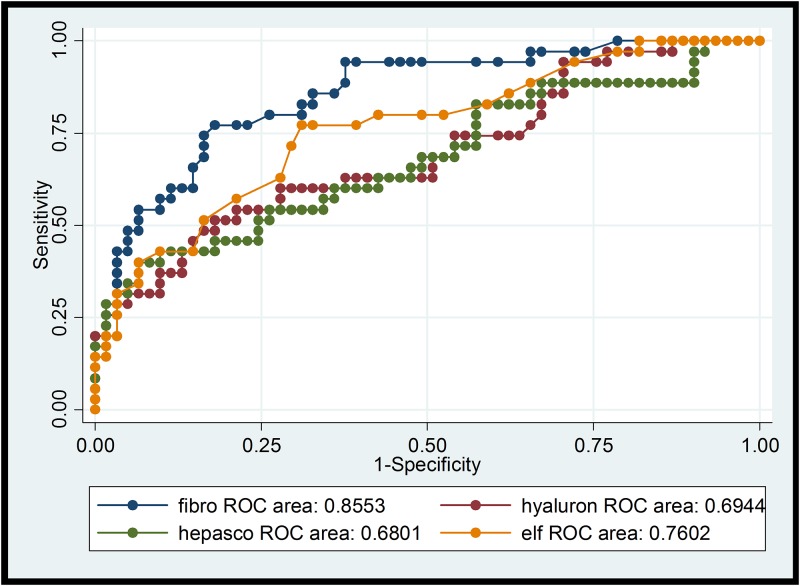
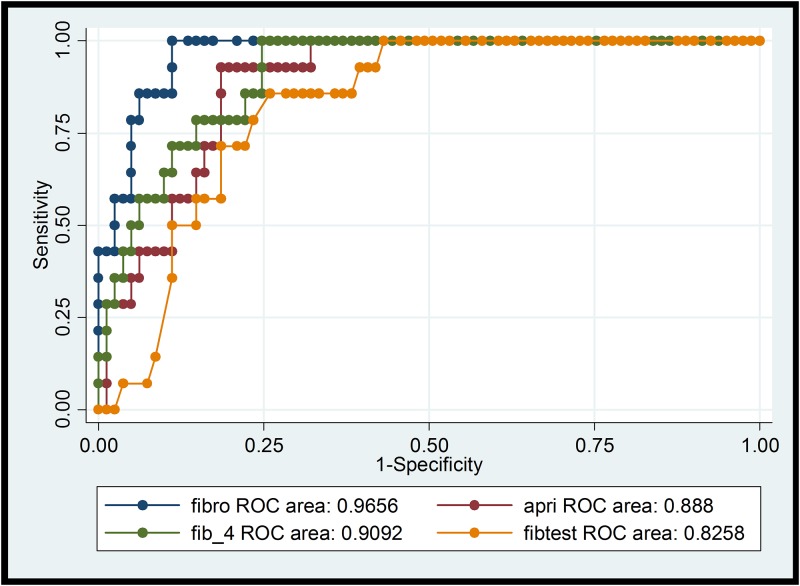
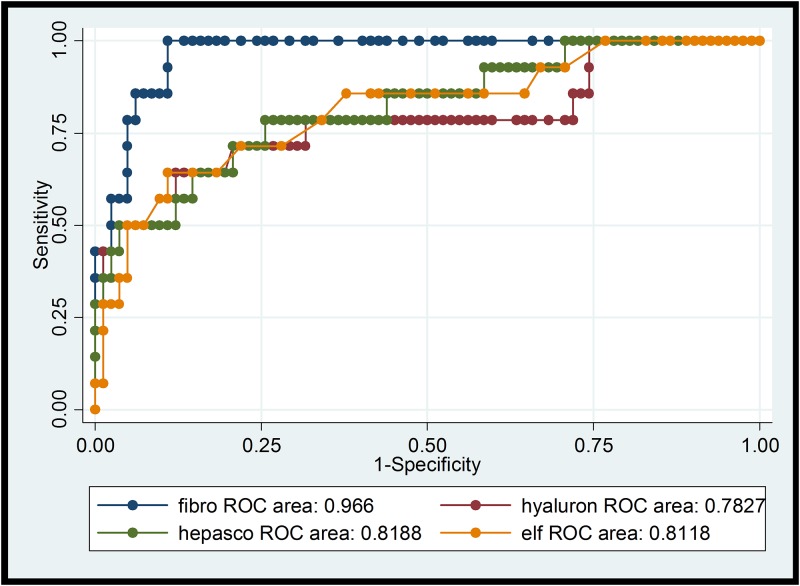
Area under the receiver operating characteristic curve (AUROC) for significant fibrosis (> = F2) in 105 participants was highest for TE (0.85), followed by FIB-4 (0.77), ELF-Test (0.77), APRI (0.76), Fibrotest (0.75), hyaluronic acid (0.70), and Hepascore (0.68). AUROC for cirrhosis (F4) was 0.97 for TE followed by FIB-4 (0.91), APRI (0.89), Fibrotest (0.84), Hepascore (0.82), ELF-Test (0.82), and hyaluronic acid (0.79). A three year follow-up was completed by 87 participants, all on antiretroviral therapy and in 20 patients who completed HCV treatment (9 with sustained virologic response). TE, APRI and Fibrotest did not significantly change during follow-up. There was weak evidence for an increase of FIB-4 (mean increase: 0.22, p = 0.07). 42 participants had a second liver biopsy: Among 38 participants with F0-F3 at baseline, 10 were progessors (1-stage increase in fibrosis, 8 participants; 2-stage, 1; 3-stage, 1). Among progressors, mean increase in TE was 3.35 kPa, in APRI 0.36, and in FIB-4 0.75. Fibrotest results did not change over 3 years.
TE was the best NIT for liver fibrosis staging in HIV/HCV co-infected patients. APRI-Score, FIB-4 Index, Fibrotest, and ELF-Test were less reliable. Routinely available APRI and FIB-4 performed as good as more expensive tests. NITs did not change significantly during a follow-up of three years, suggesting slow liver disease progression in a majority of HIV/HCV co-infected persons on antiretroviral therapy.
评估七种肝纤维化非侵入性检测(NITs)的诊断性能,并评估HIV/HCV合并感染患者随时间推移的纤维化进展情况。
将瞬时弹性成像(TE)和六项血液检测与组织病理学纤维化分期(METAVIR)进行比较。参与者接受为期三年的随访,每年进行一次NITs检测。
105名参与者中,显著纤维化(>=F2)的受试者工作特征曲线下面积(AUROC)以TE最高(0.85),其次是FIB-4(0.77)、ELF检测(0.77)、APRI(0.76)、Fibrotest(0.75)、透明质酸(0.70)和Hepascore(0.68)。肝硬化(F4)的AUROC,TE为0.97,其次是FIB-4(0.91)、APRI(0.89)、Fibrotest(0.84)、Hepascore(0.82)、ELF检测(0.82)和透明质酸(0.79)。87名参与者完成了三年随访,所有参与者均接受抗逆转录病毒治疗,20名完成HCV治疗的患者(9名获得持续病毒学应答)。随访期间,TE、APRI和Fibrotest无显著变化。有微弱证据表明FIB-4升高(平均升高:0.22,p = 0.07)。42名参与者进行了第二次肝活检:在基线时F0-F3的38名参与者中,10名病情进展(纤维化增加1期,8名参与者;2期,1名;3期,1名)。在病情进展者中,TE的平均升高为3.35 kPa,APRI为0.36,FIB-4为0.75。Fibrotest结果在3年内未发生变化。
对于HIV/HCV合并感染患者的肝纤维化分期,TE是最佳的NIT。APRI评分、FIB-4指数、Fibrotest和ELF检测可靠性较低。常规可用的APRI和FIB-4与更昂贵的检测效果相当。在三年随访期间,NITs无显著变化,这表明大多数接受抗逆转录病毒治疗的HIV/HCV合并感染患者的肝病进展缓慢。