HIV integrated services, Cipto Mangunkusumo Hospital, Jakarta, Indonesia.
Department of Internal Medicine, Faculty of Medicine Universitas Indonesia, Cipto Mangunkusumo Hospital, Diponegoro, Jakarta, 71, Indonesia.
BMC Infect Dis. 2020 May 25;20(1):372. doi: 10.1186/s12879-020-05069-5.
After successful of antiretroviral therapy, highly effective direct acting antiviral (DAA) make HCV elimination reasonable in HIV/HCV co-infected patients. However, in achieving this target, there are still barriers to start DAA treatment, particularly in the area of liver fibrosis assessment that determine the duration of therapy. We aimed to assess the diagnostic performance of APRI and FIB-4 for diagnosing cirrhosis in HIV/HCV co-infected patients using hepatic transient elastography (TE) as gold standard.
This is a retrospective study on HIV/HCV co-infected patients who concomitantly performed hepatic TE measurement, APRI, and FIB-4 evaluation before HCV treatment initiation at a tertiary hospital in Jakarta from 2014 to 2019. Sensitivity, specificity and diagnostic accuracy of indirect biomarkers for liver stiffness measurement (LSM) ≥ 12.5 kPa was determined by receiver operator characteristics curves.
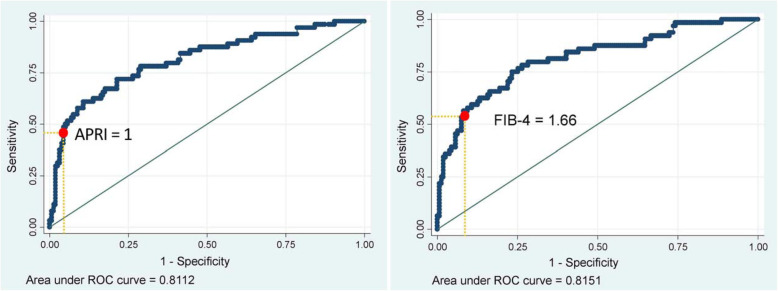
223 HIV/HCV co-infected patients on stable antiretroviral therapy were included, of whom 91.5% were male with mean age of 37 (SD 5) years. Only 28.7% of patients were classified as cirrhosis (F4). Using TE as gold standard (≥12.5 kPa), the low threshold of APRI (1) had specificity 95%, sensitivity 48.4%, correctly classified 81.6% of patients, with moderate performance, AUC at 0.72 (95% CI 0.63-0.80). The optimal cut-off of FIB-4 was 1.66 [specificity 92.5%, sensitivity 53.1%, AUC at 0.73 (95% CI 0.65-0.81)] and correctly classified 81.1% of the patients.
APRI score ≥ 1 and FIB-4 score ≥ 1.66 had moderate performance with high specificity in diagnosing cirrhosis. These biochemical markers could be used while TE is not available.
在抗逆转录病毒治疗成功后,高效直接作用抗病毒药物(DAA)使得 HCV 清除在 HIV/HCV 合并感染患者中变得合理。然而,在实现这一目标时,启动 DAA 治疗仍然存在障碍,特别是在评估肝纤维化的领域,这决定了治疗的持续时间。我们旨在评估 APRI 和 FIB-4 在使用肝瞬时弹性成像(TE)作为金标准的情况下,诊断 HIV/HCV 合并感染患者肝硬化的诊断性能。
这是一项回顾性研究,纳入了 2014 年至 2019 年在雅加达一家三级医院同时进行肝 TE 测量、APRI 和 FIB-4 评估的 HIV/HCV 合并感染患者。通过受试者工作特征曲线确定用于肝脏硬度测量(LSM)≥12.5kPa 的间接生物标志物的敏感性、特异性和诊断准确性。
共纳入 223 例接受稳定抗逆转录病毒治疗的 HIV/HCV 合并感染患者,其中 91.5%为男性,平均年龄 37(SD 5)岁。只有 28.7%的患者被分类为肝硬化(F4)。使用 TE 作为金标准(≥12.5kPa),APRI 的低值(1)具有 95%的特异性、48.4%的敏感性、正确分类 81.6%的患者,具有中等性能,AUC 为 0.72(95%CI 0.63-0.80)。FIB-4 的最佳截断值为 1.66[特异性 92.5%,敏感性 53.1%,AUC 为 0.73(95%CI 0.65-0.81)],正确分类 81.1%的患者。
APRI 评分≥1 和 FIB-4 评分≥1.66 在诊断肝硬化方面具有中等性能,特异性高。在无法获得 TE 时,可以使用这些生化标志物。