Little Simon, Beudel Martijn, Zrinzo Ludvic, Foltynie Thomas, Limousin Patricia, Hariz Marwan, Neal Spencer, Cheeran Binith, Cagnan Hayriye, Gratwicke James, Aziz Tipu Z, Pogosyan Alex, Brown Peter
Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, University of Oxford, Oxford, UK.
Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, University of Oxford, Oxford, UK Department of Neurology, University Medical Centre Groningen, University of Groningen, Groningen, The Netherlands.
J Neurol Neurosurg Psychiatry. 2016 Jul;87(7):717-21. doi: 10.1136/jnnp-2015-310972. Epub 2015 Sep 30.
INTRODUCTION & OBJECTIVES: Adaptive deep brain stimulation (aDBS) uses feedback from brain signals to guide stimulation. A recent acute trial of unilateral aDBS showed that aDBS can lead to substantial improvements in contralateral hemibody Unified Parkinson's Disease Rating Scale (UPDRS) motor scores and may be superior to conventional continuous DBS in Parkinson's disease (PD). We test whether potential benefits are retained with bilateral aDBS and in the face of concurrent medication.
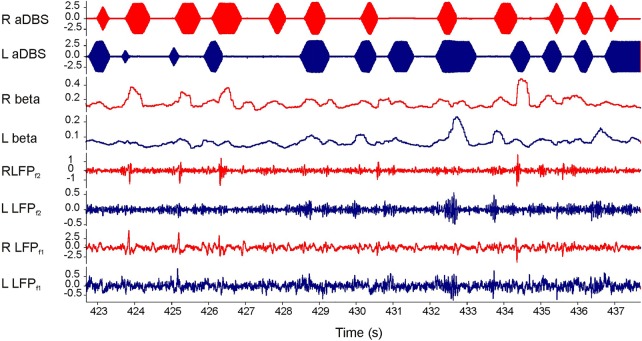
We applied bilateral aDBS in 4 patients with PD undergoing DBS of the subthalamic nucleus. aDBS was delivered bilaterally with independent triggering of stimulation according to the amplitude of β activity at the corresponding electrode. Mean stimulation voltage was 3.0±0.1 volts. Motor assessments consisted of double-blinded video-taped motor UPDRS scores that included both limb and axial features.
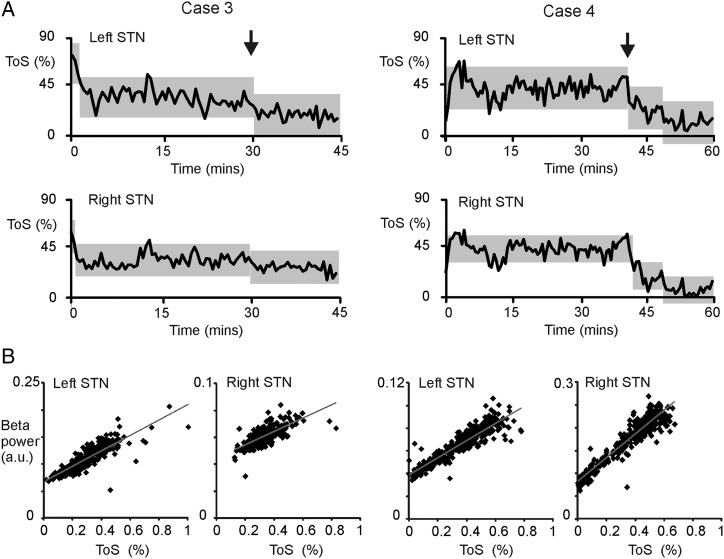
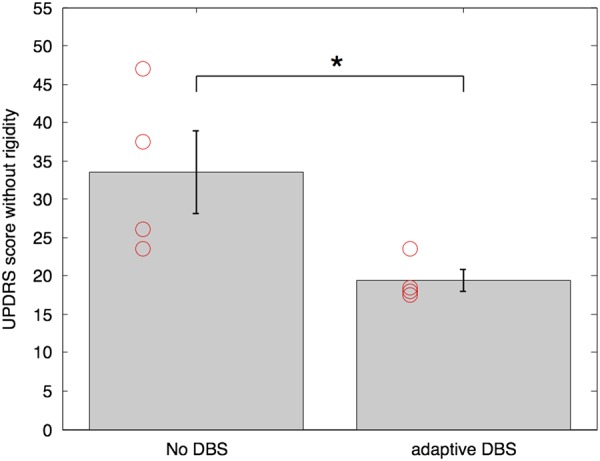
UPDRS scores were 43% (p=0.04; Cohen's d=1.62) better with aDBS than without stimulation. Motor improvement with aDBS occurred despite an average time on stimulation (ToS) of only 45%. Levodopa was well tolerated during aDBS and led to further reductions in ToS.
Bilateral aDBS can improve both axial and limb symptoms and can track the need for stimulation across drug states.
自适应深部脑刺激(aDBS)利用脑信号反馈来指导刺激。最近一项关于单侧aDBS的急性试验表明,aDBS可使对侧半侧身体的统一帕金森病评定量表(UPDRS)运动评分显著改善,且在帕金森病(PD)中可能优于传统的持续深部脑刺激。我们测试双侧aDBS以及在同时服用药物的情况下是否仍保留潜在益处。
我们对4例接受丘脑底核深部脑刺激的帕金森病患者应用双侧aDBS。根据相应电极处β活动的幅度独立触发刺激,双侧进行aDBS。平均刺激电压为3.0±0.1伏。运动评估包括双盲录像的运动UPDRS评分,涵盖肢体和轴向特征。
与无刺激相比,aDBS时UPDRS评分改善了43%(p = 0.04;科恩d值 = 1.62)。尽管平均刺激时间(ToS)仅为45%,aDBS仍带来了运动改善。在aDBS期间,左旋多巴耐受性良好,并导致ToS进一步缩短。
双侧aDBS可改善轴向和肢体症状,并可在不同药物状态下跟踪刺激需求。