Geneen Louise J, Martin Denis J, Adams Nicola, Clarke Clare, Dunbar Martin, Jones Derek, McNamee Paul, Schofield Pat, Smith Blair H
Division of Population Health Sciences, University of Dundee, Dundee, UK.
Institute of Health and Social Care, Teesside University, Middlesbrough, UK.
Syst Rev. 2015 Oct 1;4:132. doi: 10.1186/s13643-015-0120-5.
Chronic pain can contribute to disability, depression, anxiety, sleep disturbances, poor quality of life and increased health care costs, with close to 20 % of the adult population in Europe reporting chronic pain. To empower the person to self-manage, it is advocated that education and training about the nature of pain and its effects and how to live with pain is provided. The objective of this review is to determine the level of evidence for education to facilitate knowledge about chronic pain, delivered as a stand-alone intervention for adults, to reduce pain and disability.
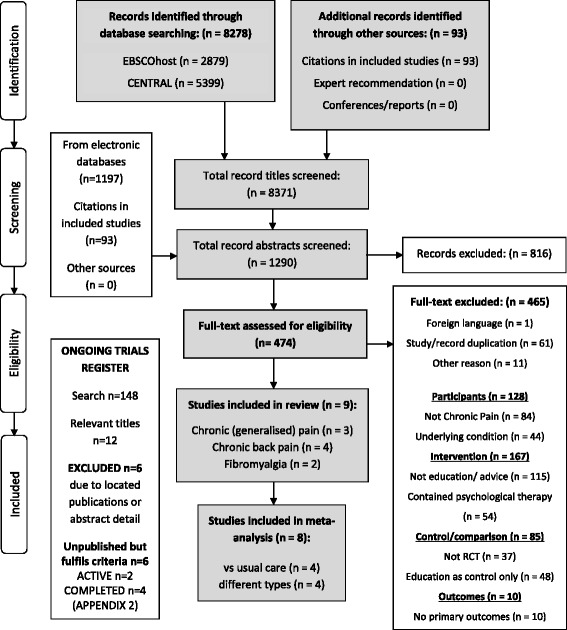
We identified randomised controlled trials of educational intervention for chronic pain by searching CENTRAL, MEDLINE, EMBASE and ongoing trials registries (inception to December 2013). Main inclusion criteria were (1) pain >3 months; (2) study design that allowed isolation of effects of education and (3) measures of pain or disability. Two reviewers independently screened and appraised each study.
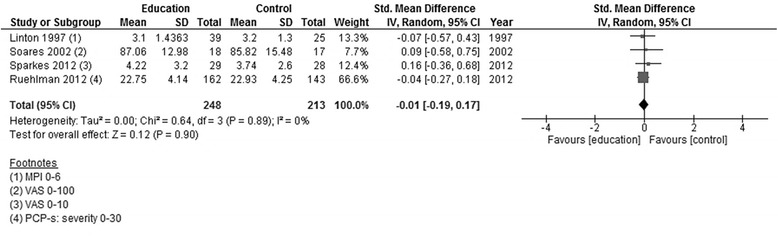
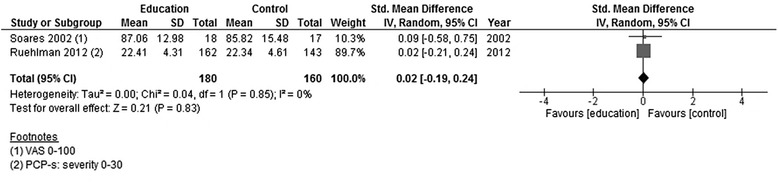
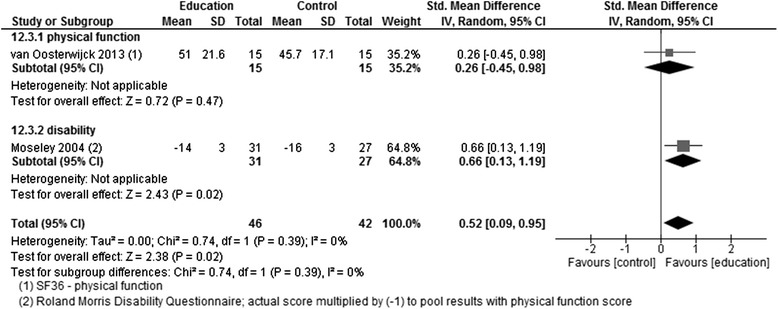
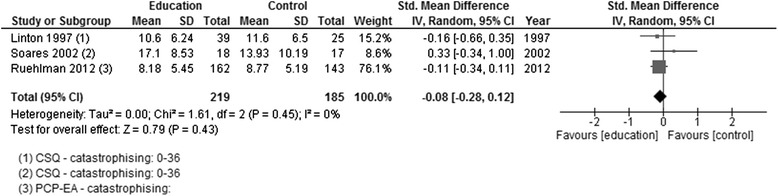
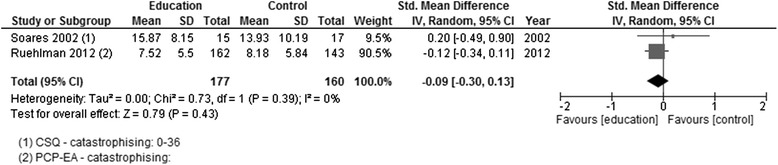
Nine studies were analysed. Pooled data from five studies, where the comparator group was usual care, showed no improvement in pain or disability. In the other four studies, comparing different types of education, there was no evidence for an improvement in pain; although, there was evidence (from one study) of a decrease in disability with a particular form of education-pain neurophysiology education (PNE). Post-hoc analysis of psychosocial outcomes reported in the studies showed evidence of a reduction in catastrophising and an increase of knowledge about pain following PNE.
The evidence base is limited by the small numbers of studies, their relatively small sample sizes, and the diversity in types of education studied. From that limited evidence, the only support for this type of education is for PNE, though it is insufficiently strong to recommend conclusively that PNE should be delivered as a stand-alone intervention. It therefore remains sensible to recommend that education be delivered in conjunction with other pain management approaches as we cannot confidently conclude that education alone is effective in reducing pain intensity or related disability in chronic pain in adults.
慢性疼痛会导致残疾、抑郁、焦虑、睡眠障碍、生活质量下降以及医疗费用增加,欧洲近20%的成年人口报告患有慢性疼痛。为了使患者能够自我管理,提倡提供有关疼痛的性质及其影响以及如何与疼痛共处的教育和培训。本综述的目的是确定作为成人独立干预措施的慢性疼痛教育促进知识、减轻疼痛和残疾的证据水平。
我们通过检索Cochrane系统评价数据库、医学期刊数据库、荷兰医学文摘数据库和正在进行的试验注册库(从开始到2013年12月),确定了慢性疼痛教育干预的随机对照试验。主要纳入标准为:(1)疼痛持续>3个月;(2)允许分离教育效果的研究设计;(3)疼痛或残疾的测量指标。两名评审员独立筛选和评估每项研究。
共分析了9项研究。五项研究的汇总数据显示,与常规护理相比,疼痛或残疾没有改善。在其他四项比较不同类型教育的研究中,没有证据表明疼痛有所改善;不过,有证据(来自一项研究)表明,一种特定形式的教育——疼痛神经生理学教育(PNE)可降低残疾程度。对研究中报告的心理社会结果进行的事后分析表明,PNE后灾难化思维减少,有关疼痛的知识增加。
证据基础受到研究数量少、样本量相对较小以及所研究教育类型多样性的限制。从有限的证据来看,对这类教育的唯一支持是针对PNE,但力度不足以确凿推荐将PNE作为独立干预措施。因此,建议将教育与其他疼痛管理方法结合使用仍然是明智的,因为我们不能肯定地得出结论,仅教育就能有效降低成人慢性疼痛的强度或相关残疾。