Bewersdorf Jan Philipp, Hautmann Oliver, Kofink Daniel, Abdul Khalil Alizan, Zainal Abidin Imran, Loch Alexander
Departments of aSurgery bMedicine, University Malaya Medical Centre, Kuala Lumpur, Malaysia cLaboratory of Experimental Cardiology, Department of Cardiology, Division of Heart and Lung, University Medical Center Utrecht, Utrecht, The Netherlands.
Eur J Emerg Med. 2017 Jun;24(3):170-175. doi: 10.1097/MEJ.0000000000000344.
The aim of the study was to identify covariates associated with 28-day mortality in septic patients admitted to the emergency department and derive and validate a score that stratifies mortality risk utilizing parameters that are readily available.
Patients with an admission diagnosis of suspected or confirmed infection and fulfilling at least two criteria for severe inflammatory response syndrome were included in this study. Patients' characteristics, vital signs, and laboratory values were used to identify prognostic factors for mortality. A scoring system was derived and validated. The primary outcome was the 28-day mortality rate.
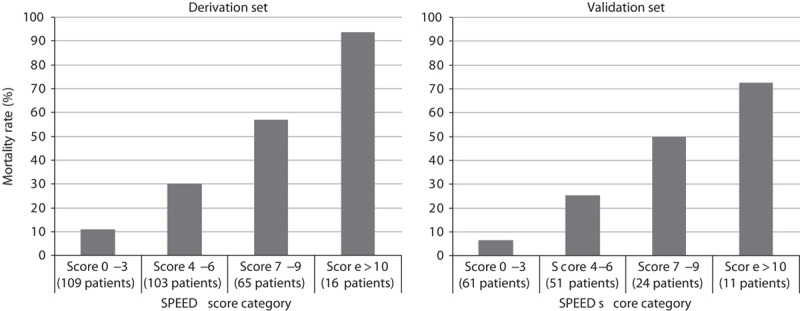
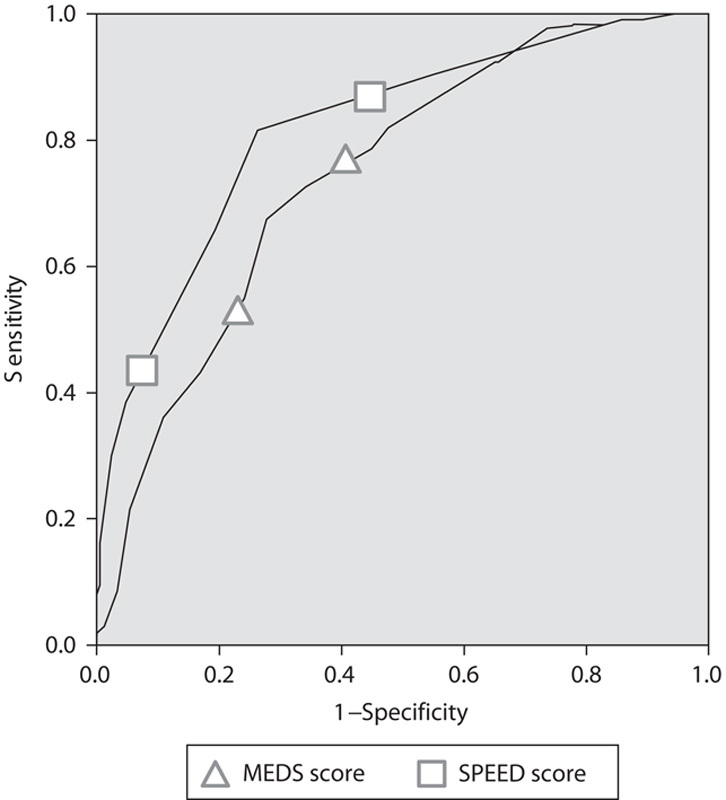
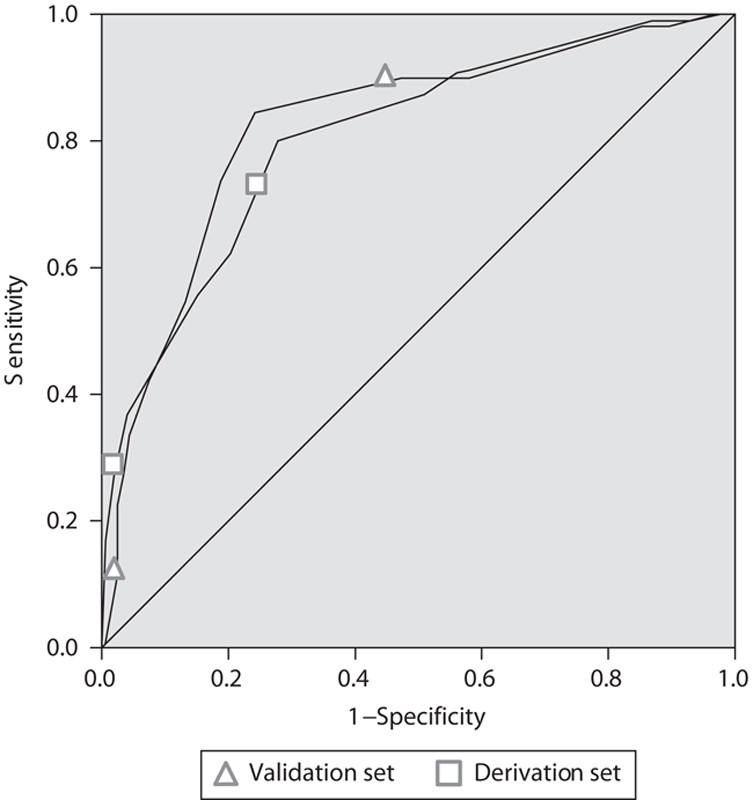
A total of 440 patients were included in the study. The 28-day hospital mortality rate was 32.4 and 25.2% for the derivation (293 patients) and validation (147 patients) sets, respectively. Factors associated with a higher mortality were immune-suppressed state (odds ratio 4.7; 95% confidence interval 2.0-11.4), systolic blood pressure on arrival less than 90 mmHg (3.8; 1.7-8.3), body temperature less than 36.0°C (4.1; 1.3-12.9), oxygen saturation less than 90% (2.3; 1.1-4.8), hematocrit less than 0.38 (3.1; 1.6-5.9), blood pH less than 7.35 (2.0; 1.04-3.9), lactate level more than 2.4 mmol/l (2.27; 1.2-4.2), and pneumonia as the source of infection (2.7; 1.5-5.0). The area under the receiver operating characteristic curve was 0.81 (0.75-0.86) in the derivation and 0.81 (0.73-0.90) in the validation set. The SPEED (sepsis patient evaluation in the emergency department) score performed better (P=0.02) than the Mortality in Emergency Department Sepsis score when applied to the complete study population with an area under the curve of 0.81 (0.76-0.85) as compared with 0.74 (0.70-0.79).
The SPEED score predicts 28-day mortality in septic patients. It is simple and its predictive value is comparable to that of other scoring systems.
本研究旨在确定急诊科收治的脓毒症患者28天死亡率的相关协变量,并利用易于获取的参数得出并验证一个对死亡风险进行分层的评分系统。
本研究纳入入院诊断为疑似或确诊感染且至少符合两条严重炎症反应综合征标准的患者。患者的特征、生命体征和实验室检查值用于确定死亡的预后因素。得出并验证了一个评分系统。主要结局为28天死亡率。
本研究共纳入440例患者。在推导集(293例患者)和验证集(147例患者)中,28天医院死亡率分别为32.4%和25.2%。与较高死亡率相关的因素包括免疫抑制状态(比值比4.7;95%置信区间2.0 - 11.4)、入院时收缩压低于90 mmHg(3.8;1.7 - 8.3)、体温低于36.0°C(4.1;1.3 - 12.9)、氧饱和度低于90%(2.3;1.1 - 4.8)、血细胞比容低于0.38(3.1;1.6 - 5.9)、血液pH低于7.35(2.0;1.04 - 3.9)、乳酸水平高于2.4 mmol/L(2.27;1.2 - 4.2)以及肺炎作为感染源(2.7;1.5 - 5.0)。在推导集中,受试者工作特征曲线下面积为0.81(0.75 - 0.86),在验证集中为0.81(0.73 - 0.90)。当应用于完整研究人群时,SPEED(急诊科脓毒症患者评估)评分(曲线下面积为0.81(0.76 - 0.85))比急诊科脓毒症死亡率评分(曲线下面积为0.74(0.70 - 0.79))表现更好(P = 0.02)。
SPEED评分可预测脓毒症患者的28天死亡率。它简单易行,其预测价值与其他评分系统相当。