Herbert Annie, Gilbert Ruth, González-Izquierdo Arturo, Pitman Alexandra, Li Leah
Population, Policy & Practice Programme, Institute of Child Health, University College London, London, United Kingdom.
Farr Institute of Health Informatics Research, Department of Epidemiology and Public Health, University College London, London, United Kingdom.
PLoS Med. 2015 Dec 29;12(12):e1001931. doi: 10.1371/journal.pmed.1001931. eCollection 2015 Dec.
Hospitalisation for adversity-related injury (violent, drug/alcohol-related, or self-inflicted injury) has been described as a "teachable moment", when intervention may reduce risks of further harm. Which adolescents are likely to benefit most from intervention strongly depends on their long-term risks of harm. We compared 10-y risks of mortality and re-admission after adversity-related injury with risks after accident-related injury.
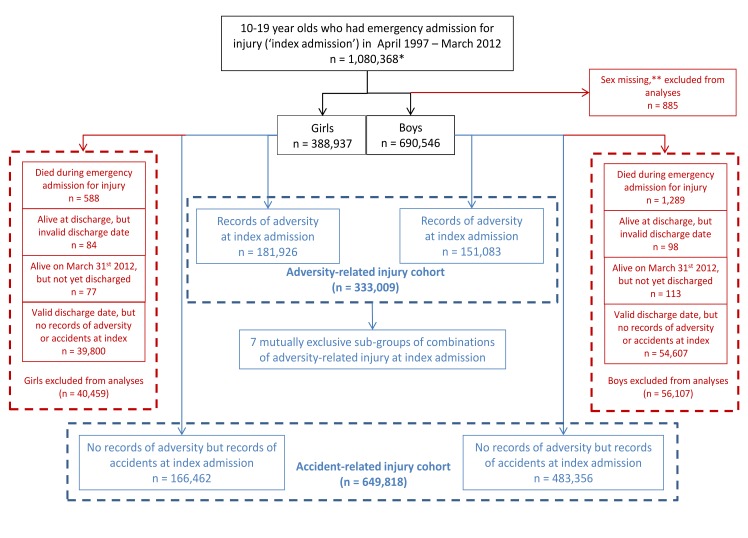
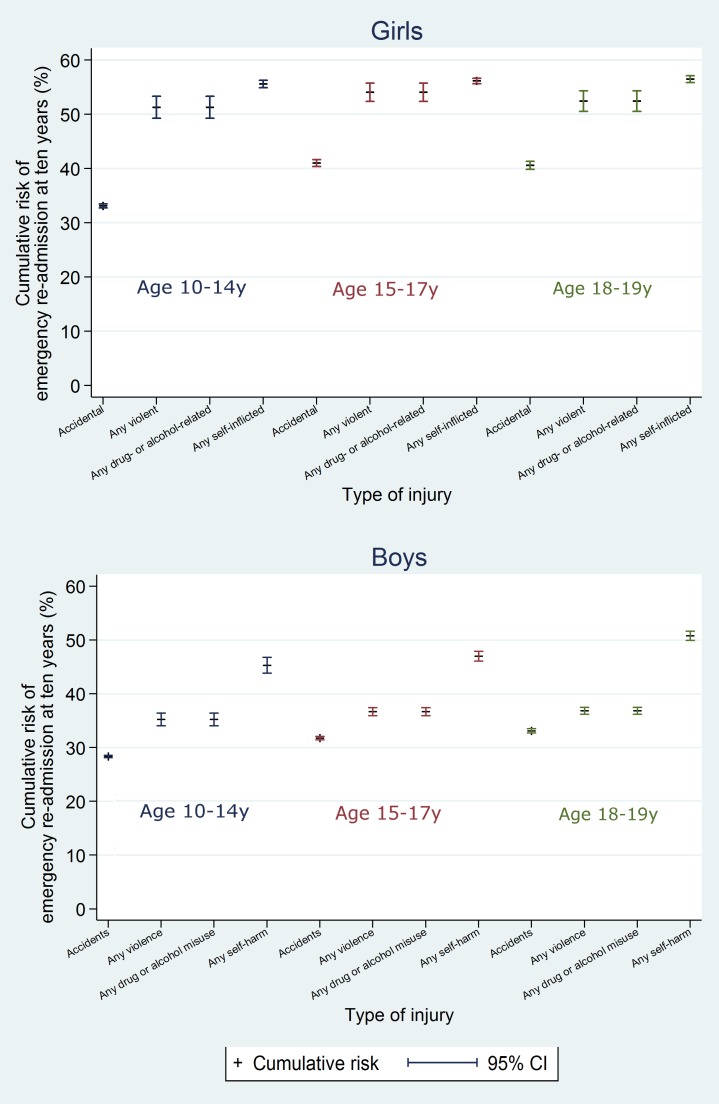
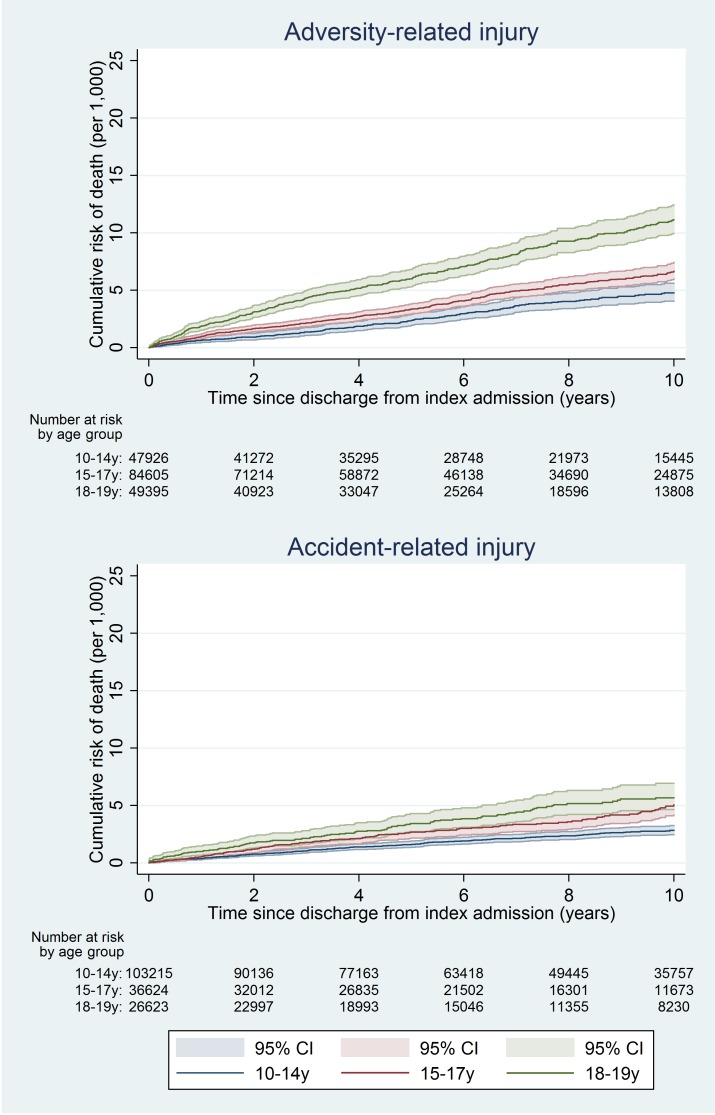
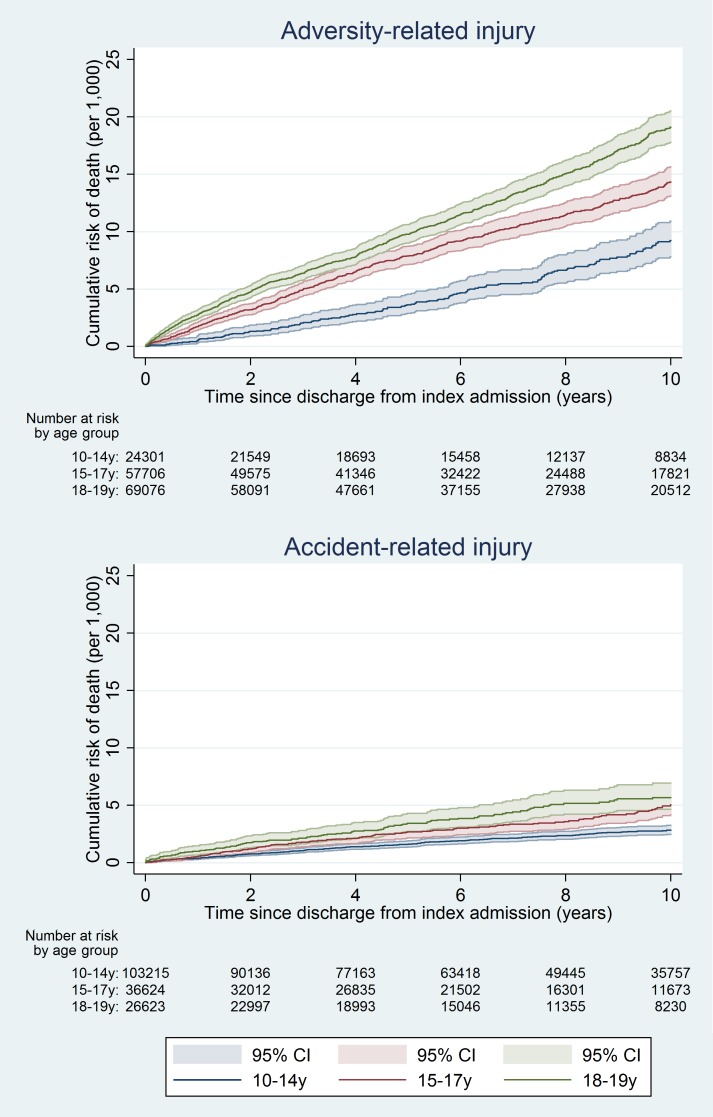
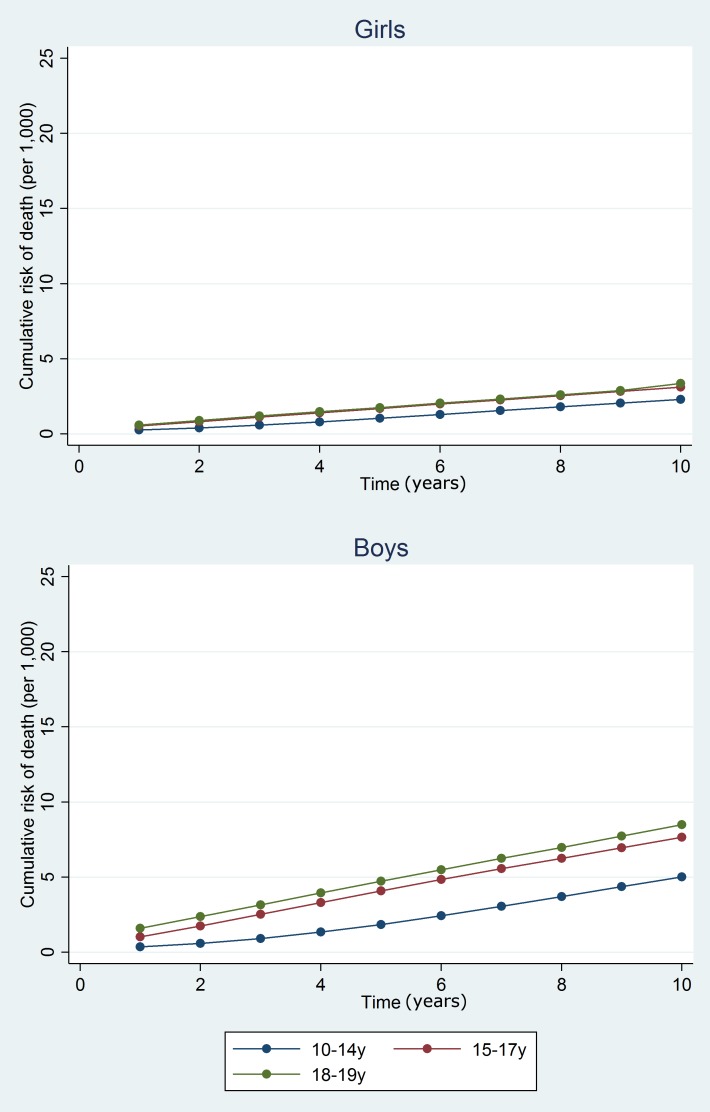
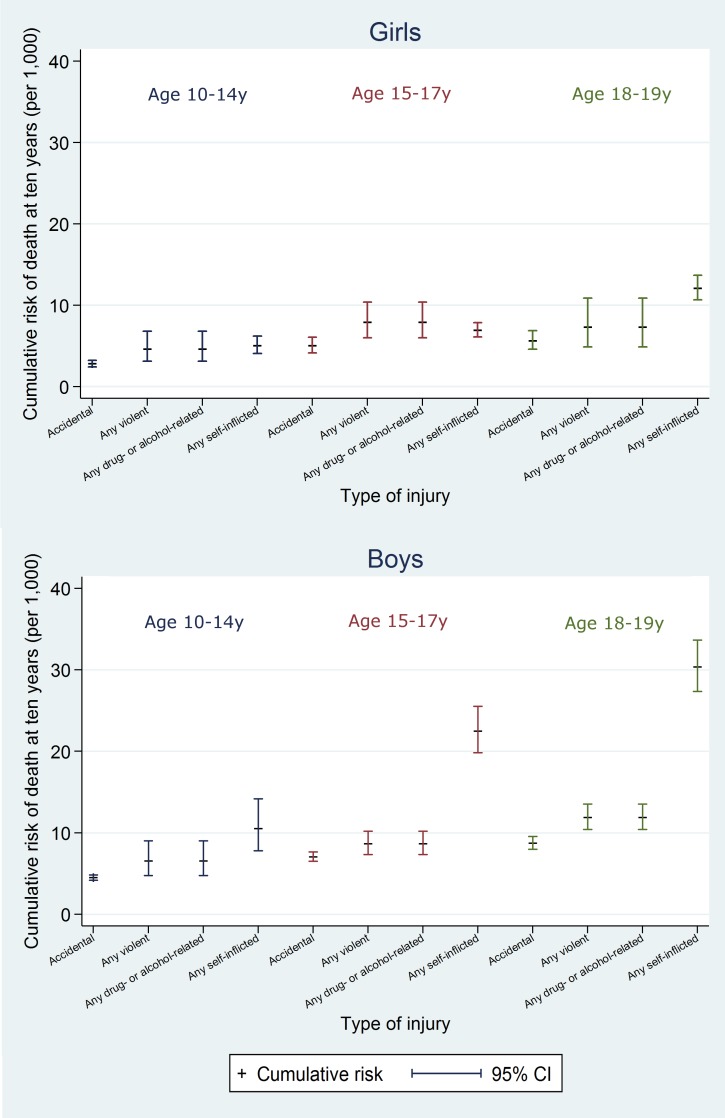
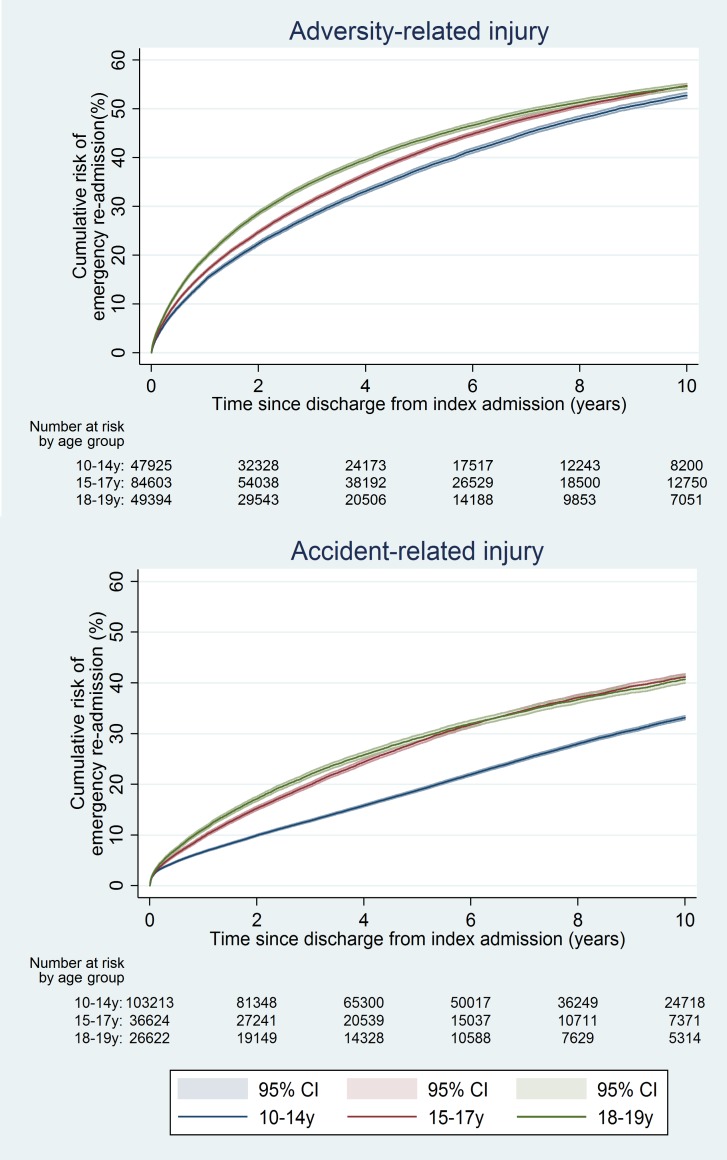
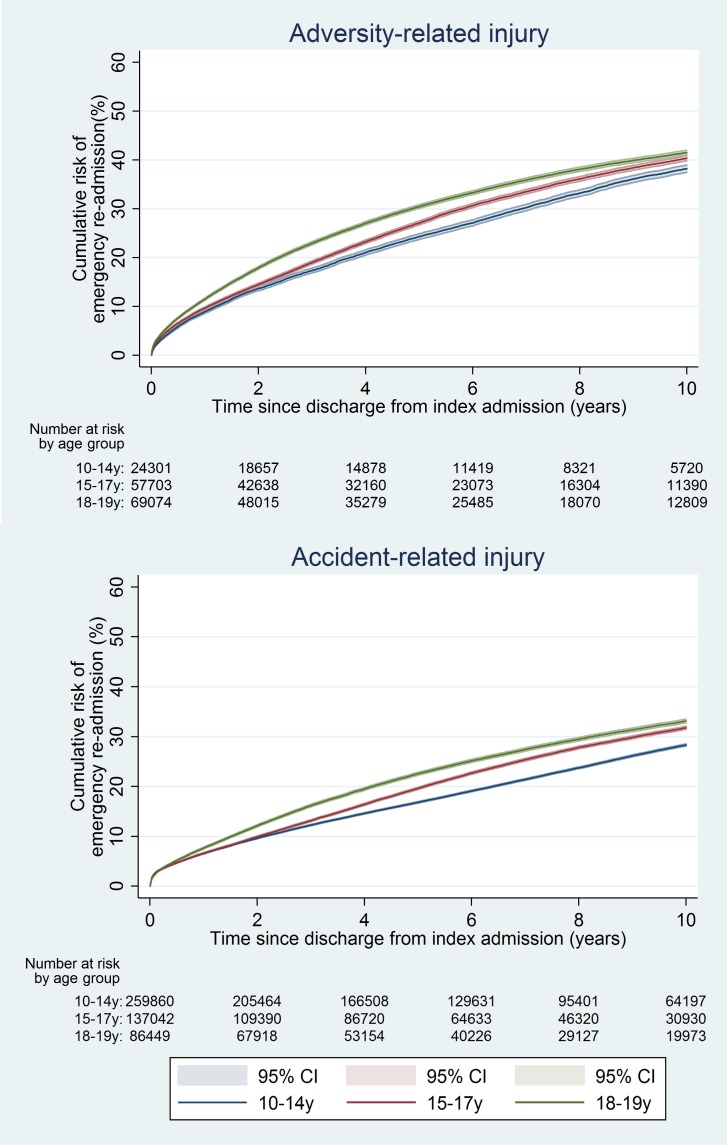
We analysed National Health Service admissions data for England (1 April 1997-31 March 2012) for 10-19 y olds with emergency admissions for adversity-related injury (violent, drug/alcohol-related, or self-inflicted injury; n = 333,009) or for accident-related injury (n = 649,818). We used Kaplan-Meier estimates and Cox regression to estimate and compare 10-y post-discharge risks of death and emergency re-admission. Among adolescents discharged after adversity-related injury, one in 137 girls and one in 64 boys died within 10 y, and 54.2% of girls and 40.5% of boys had an emergency re-admission, with rates being highest for 18-19 y olds. Risks of death were higher than in adolescents discharged after accident-related injury (girls: age-adjusted hazard ratio 1.61, 95% CI 1.43-1.82; boys: 2.13, 95% CI 1.98-2.29), as were risks of re-admission (girls: 1.76, 95% CI 1.74-1.79; boys: 1.41, 95% CI 1.39-1.43). Risks of death and re-admission were increased after all combinations of violent, drug/alcohol-related, and self-inflicted injury, but particularly after any drug/alcohol-related or self-inflicted injury (i.e., with/without violent injury), for which age-adjusted hazard ratios for death in boys ranged from 1.67 to 5.35, compared with 1.25 following violent injury alone (girls: 1.09 to 3.25, compared with 1.27). The main limitation of the study was under-recording of adversity-related injuries and misclassification of these cases as accident-related injuries. This misclassification would attenuate the relative risks of death and re-admission for adversity-related compared with accident-related injury.
Adolescents discharged after an admission for violent, drug/alcohol-related, or self-inflicted injury have increased risks of subsequent harm up to a decade later. Introduction of preventive strategies for reducing subsequent harm after admission should be considered for all types of adversity-related injury, particularly for older adolescents.
因与逆境相关的伤害(暴力、药物/酒精相关或自残伤害)而住院被描述为一个“可教育的时机”,此时进行干预可能会降低进一步伤害的风险。哪些青少年最有可能从干预中受益很大程度上取决于他们长期的伤害风险。我们比较了与逆境相关伤害后10年的死亡率和再入院风险与事故相关伤害后的风险。
我们分析了英格兰国民健康服务体系(1997年4月1日至2012年3月31日)的入院数据,对象为10至19岁因与逆境相关伤害(暴力、药物/酒精相关或自残伤害;n = 333,009)或事故相关伤害(n = 649,818)而紧急入院的青少年。我们使用Kaplan-Meier估计法和Cox回归来估计和比较出院后10年的死亡风险和紧急再入院风险。在因与逆境相关伤害而出院的青少年中,137名女孩中有1名、64名男孩中有1名在10年内死亡,54.2%的女孩和40.5%的男孩有紧急再入院情况,18至19岁的青少年发生率最高。死亡风险高于事故相关伤害后出院的青少年(女孩:年龄调整后的风险比为1.61,95%置信区间为1.43 - 1.82;男孩:2.13,95%置信区间为1.98 - 2.29),再入院风险也是如此(女孩:1.76,95%置信区间为1.74 - 1.79;男孩:1.41,95%置信区间为1.39 - 1.43)。在暴力、药物/酒精相关和自残伤害的所有组合后,死亡和再入院风险均增加,但特别是在任何药物/酒精相关或自残伤害后(即有/无暴力伤害),男孩因这些伤害导致死亡的年龄调整后风险比范围为1.67至5.35,而仅暴力伤害后的风险比为1.25(女孩:1.09至3.25,而仅暴力伤害后的风险比为1.27)。该研究的主要局限性是与逆境相关伤害的记录不足以及这些病例被误分类为事故相关伤害。这种误分类会减弱与事故相关伤害相比,与逆境相关伤害的死亡和再入院相对风险。
因暴力、药物/酒精相关或自残伤害入院后出院的青少年在长达十年后有更高的后续伤害风险。对于所有类型的与逆境相关伤害,尤其是年龄较大的青少年,应考虑引入预防策略以减少入院后的后续伤害。