Sariaslan Amir, Sharp David J, D'Onofrio Brian M, Larsson Henrik, Fazel Seena
Department of Psychiatry, University of Oxford, Warneford Hospital, Oxford, United Kingdom.
Computational, Cognitive and Clinical Neuroimaging Laboratory, Imperial College, London, United Kingdom.
PLoS Med. 2016 Aug 23;13(8):e1002103. doi: 10.1371/journal.pmed.1002103. eCollection 2016 Aug.
Traumatic brain injury (TBI) is the leading cause of disability and mortality in children and young adults worldwide. It remains unclear, however, how TBI in childhood and adolescence is associated with adult mortality, psychiatric morbidity, and social outcomes.
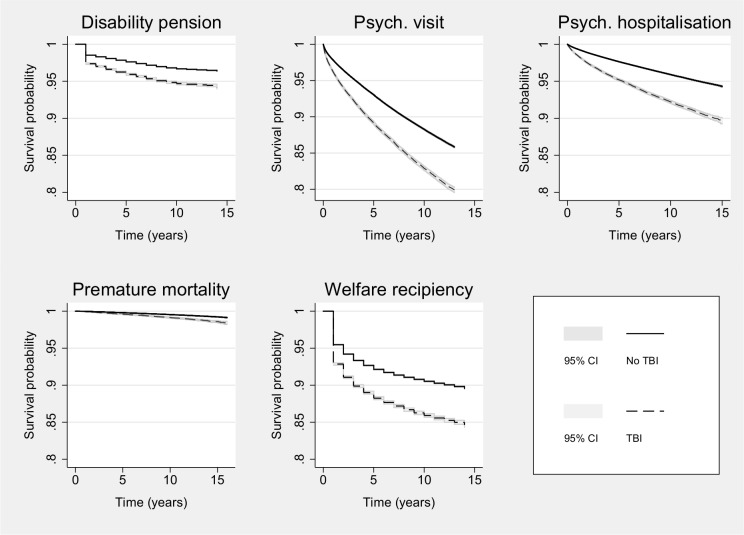
In a Swedish birth cohort between 1973 and 1985 of 1,143,470 individuals, we identified all those who had sustained at least one TBI (n = 104,290 or 9.1%) up to age 25 y and their unaffected siblings (n = 68,268) using patient registers. We subsequently assessed these individuals for the following outcomes using multiple national registries: disability pension, specialist diagnoses of psychiatric disorders and psychiatric inpatient hospitalisation, premature mortality (before age 41 y), low educational attainment (not having achieved secondary school qualifications), and receiving means-tested welfare benefits. We used logistic and Cox regression models to quantify the association between TBI and specified adverse outcomes on the individual level. We further estimated population attributable fractions (PAF) for each outcome measure. We also compared differentially exposed siblings to account for unobserved genetic and environmental confounding. In addition to relative risk estimates, we examined absolute risks by calculating prevalence and Kaplan-Meier estimates. In complementary analyses, we tested whether the findings were moderated by injury severity, recurrence, and age at first injury (ages 0-4, 5-9, 6-10, 15-19, and 20-24 y). TBI exposure was associated with elevated risks of impaired adult functioning across all outcome measures. After a median follow-up period of 8 y from age 26 y, we found that TBI contributed to absolute risks of over 10% for specialist diagnoses of psychiatric disorders and low educational attainment, approximately 5% for disability pension, and 2% for premature mortality. The highest relative risks, adjusted for sex, birth year, and birth order, were found for psychiatric inpatient hospitalisation (adjusted relative risk [aRR] = 2.0; 95% CI: 1.9-2.0; 6,632 versus 37,095 events), disability pension (aRR = 1.8; 95% CI: 1.7-1.8; 4,691 versus 29,778 events), and premature mortality (aRR = 1.7; 95% CI: 1.6-1.9; 799 versus 4,695 events). These risks were only marginally attenuated when the comparisons were made with their unaffected siblings, which implies that the effects of TBI were consistent with a causal inference. A dose-response relationship was observed with injury severity. Injury recurrence was also associated with higher risks-in particular, for disability pension we found that recurrent TBI was associated with a 3-fold risk increase (aRR = 2.6; 95% CI: 2.4-2.8) compared to a single-episode TBI. Higher risks for all outcomes were observed for those who had sustained their first injury at an older age (ages 20-24 y) with more than 25% increase in relative risk across all outcomes compared to the youngest age group (ages 0-4 y). On the population level, TBI explained between 2%-6% of the variance in the examined outcomes. Using hospital data underestimates milder forms of TBI, but such misclassification bias suggests that the reported estimates are likely conservative. The sibling-comparison design accounts for unmeasured familial confounders shared by siblings, including half of their genes. Thus, residual genetic confounding remains a possibility but will unlikely alter our main findings, as associations were only marginally attenuated within families.
Given our findings, which indicate potentially causal effects between TBI exposure in childhood and later impairments across a range of health and social outcomes, age-sensitive clinical guidelines should be considered and preventive strategies should be targeted at children and adolescents.
创伤性脑损伤(TBI)是全球儿童和青年致残和致死的主要原因。然而,儿童期和青少年期的创伤性脑损伤如何与成人死亡率、精神疾病发病率和社会结局相关联仍不清楚。
在瑞典1973年至1985年出生队列中的1143470名个体中,我们使用患者登记册确定了所有在25岁之前至少遭受过一次创伤性脑损伤的个体(n = 104290或9.1%)及其未受影响的兄弟姐妹(n = 68268)。随后,我们使用多个国家登记册对这些个体进行以下结局评估:残疾抚恤金、精神疾病专科诊断和精神科住院治疗、过早死亡(41岁之前)、低教育程度(未获得中学学历)以及领取经过经济状况调查的福利金。我们使用逻辑回归和Cox回归模型在个体层面量化创伤性脑损伤与特定不良结局之间的关联。我们还估计了每个结局指标的人群归因分数(PAF)。我们还比较了暴露程度不同的兄弟姐妹,以考虑未观察到的遗传和环境混杂因素。除了相对风险估计外,我们还通过计算患病率和Kaplan-Meier估计值来检查绝对风险。在补充分析中,我们测试了研究结果是否受到损伤严重程度、复发情况和首次受伤年龄(0 - 4岁、5 - 9岁、6 - 10岁、15 - 19岁和20 - 24岁)的影响。创伤性脑损伤暴露与所有结局指标中成人功能受损风险升高相关。从26岁起经过中位随访期8年后,我们发现创伤性脑损伤导致精神疾病专科诊断和低教育程度的绝对风险超过10%,残疾抚恤金约为5%,过早死亡约为2%。在对性别、出生年份和出生顺序进行调整后,精神科住院治疗的相对风险最高(调整后相对风险[aRR] = 2.0;95% CI:1.9 - 2.0;6632例与37095例事件),残疾抚恤金(aRR = 1.8;95% CI:1.7 - 1.8;4691例与29778例事件),过早死亡(aRR = 1.7;95% CI:1.6 - 1.9;799例与4695例事件)。当与未受影响的兄弟姐妹进行比较时,这些风险仅略有减弱,这意味着创伤性脑损伤的影响与因果推断一致。观察到与损伤严重程度存在剂量反应关系。损伤复发也与更高风险相关——特别是对于残疾抚恤金,我们发现复发性创伤性脑损伤与单次创伤性脑损伤相比风险增加了3倍(aRR = 2.6;95% CI:2.4 - 2.8)。首次受伤年龄较大(20 - 24岁)的个体在所有结局方面的风险更高,与最年轻年龄组(0 - 4岁)相比,所有结局的相对风险增加超过25%。在人群层面,创伤性脑损伤解释了所检查结局中2% - 6%的变异。使用医院数据会低估较轻形式的创伤性脑损伤,但这种错误分类偏差表明报告的估计值可能较为保守。兄弟姐妹比较设计考虑了兄弟姐妹共有的未测量家族混杂因素,包括他们一半的基因。因此,残留的遗传混杂因素仍然有可能,但不太可能改变我们的主要发现,因为家庭内部的关联仅略有减弱。
鉴于我们的研究结果表明儿童期创伤性脑损伤暴露与一系列健康和社会结局的后期损害之间可能存在因果效应,应考虑制定年龄敏感的临床指南,并针对儿童和青少年制定预防策略。