Department of Medicine, University of California San Francisco School of Medicine; Department of Global Health, Academic Medical Center, Amsterdam Institute for Global Health and Development, University of Amsterdam, The Netherlands; Faculty of Health Sciences, The Desmond Tutu HIV Centre, Institute of Infectious Disease and Molecular Medicine, University of Cape Town, South Africa.
Faculty of Health Sciences, The Desmond Tutu HIV Centre, Institute of Infectious Disease and Molecular Medicine, University of Cape Town, South Africa; Department of Clinical Research, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, United Kingdom; Department of Medicine, Faculty of Health Sciences, University of Cape Town.
Open Forum Infect Dis. 2015 Nov 12;2(4):ofv173. doi: 10.1093/ofid/ofv173. eCollection 2015 Dec.
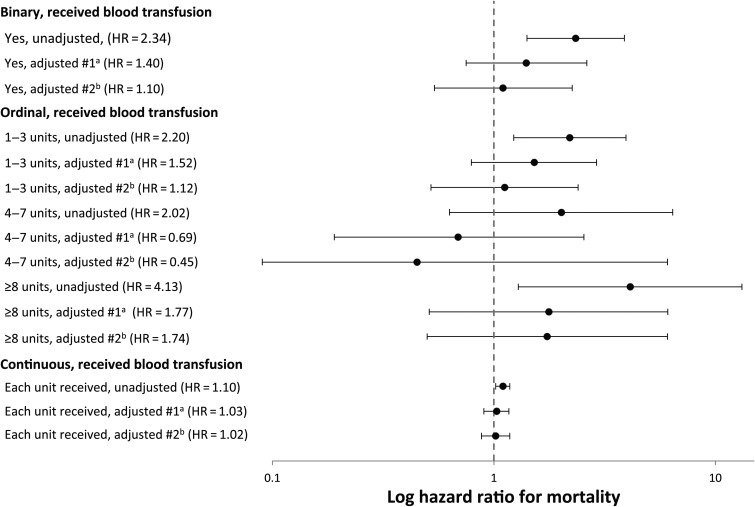
Background. Morbidity and mortality remain high among hospitalized patients infected with human immunodeficiency virus (HIV) in sub-Saharan Africa despite widespread availability of antiretroviral therapy. Severe anemia is likely one important driver, and some evidence suggests that blood transfusions may accelerate HIV progression and paradoxically increase short-term mortality. We investigated the relationship between anemia, blood transfusions, and mortality in a South African district hospital. Methods. Unselected consecutive HIV-infected adults requiring acute medical admission to a Cape Town township district hospital were recruited. Admission hemoglobin concentrations were used to classify anemia severity according to World Health Organization/AIDS Clinical Trials Group criteria. Vital status was determined at 90 days, and Cox regression analyses were used to determine independent predictors of mortality. Results. Of 585 HIV-infected patients enrolled, 578 (98.8%) were included in the analysis. Anemia was detected in 84.8% of patients and was severe (hemoglobin, 6.5-7.9 g/dL) or life-threatening (hemoglobin, <6.5 g/dL) in 17.3% and 13.3%, respectively. Within 90 days of the date of admission, 13.5% (n = 78) patients received at least 1 blood transfusion with red cell concentrate and 77 (13.3%) patients died. In univariable analysis, baseline hemoglobin and receipt of blood transfusion were associated with increased mortality risk. However, in multivariable analysis, neither hemoglobin nor receipt of a blood transfusion were independently associated with greater mortality risk. Acquired immune deficiency syndrome-defining illnesses other than tuberculosis and impaired renal function independently predicted mortality. Conclusions. Newly admitted HIV-infected adults had a high prevalence of severe or life-threatening anemia and blood transfusions were frequently required. However, after adjustment for confounders, blood transfusions did not confer an increased mortality risk.
尽管抗逆转录病毒疗法在撒哈拉以南非洲广泛应用,但感染人类免疫缺陷病毒 (HIV) 的住院患者的发病率和死亡率仍然很高。严重贫血可能是一个重要的驱动因素,一些证据表明输血可能会加速 HIV 进展,并反常地增加短期死亡率。我们研究了南非一家地区医院中贫血、输血和死亡率之间的关系。
我们招募了无选择的、连续的、需要急性内科住院治疗的开普敦城镇地区医院的 HIV 感染成人患者。根据世界卫生组织/艾滋病临床试验组的标准,入院时的血红蛋白浓度用于分类贫血严重程度。在 90 天确定存活状态,并使用 Cox 回归分析确定死亡率的独立预测因素。
在纳入的 585 名 HIV 感染患者中,578 名(98.8%)被纳入分析。84.8%的患者存在贫血,17.3%和 13.3%的患者贫血严重(血红蛋白 6.5-7.9 g/dL)或危及生命(血红蛋白 <6.5 g/dL)。在入院日期后的 90 天内,13.5%(n = 78)的患者至少接受了 1 次红细胞浓缩物输血,77 名(13.3%)患者死亡。在单变量分析中,基线血红蛋白和输血与更高的死亡风险相关。然而,在多变量分析中,血红蛋白和输血均与更高的死亡率无关。除结核病外的获得性免疫缺陷综合征定义性疾病和肾功能受损独立预测死亡率。
新入院的 HIV 感染成年患者严重或危及生命的贫血患病率较高,且经常需要输血。然而,在调整混杂因素后,输血并未增加死亡率风险。