Silva Romesh, Amouzou Agbessi, Munos Melinda, Marsh Andrew, Hazel Elizabeth, Victora Cesar, Black Robert, Bryce Jennifer
Institute for International Programs, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
Economic and Social Commission for Western Asia, United Nations, Beirut, Lebanon.
PLoS One. 2016 Jan 5;11(1):e0144662. doi: 10.1371/journal.pone.0144662. eCollection 2016.
Most low-income countries lack complete and accurate vital registration systems. As a result, measures of under-five mortality rates rely mostly on household surveys. In collaboration with partners in Ethiopia, Ghana, Malawi, and Mali, we assessed the completeness and accuracy of reporting of births and deaths by community-based health workers, and the accuracy of annualized under-five mortality rate estimates derived from these data. Here we report on results from Ethiopia, Malawi and Mali.
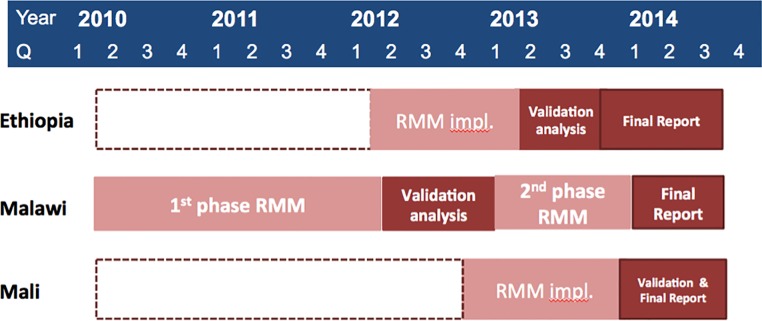
In all three countries, community health workers (CHWs) were trained, equipped and supported to report pregnancies, births and deaths within defined geographic areas over a period of at least fifteen months. In-country institutions collected these data every month. At each study site, we administered a full birth history (FBH) or full pregnancy history (FPH), to women of reproductive age via a census of households in Mali and via household surveys in Ethiopia and Malawi. Using these FBHs/FPHs as a validation data source, we assessed the completeness of the counts of births and deaths and the accuracy of under-five, infant, and neonatal mortality rates from the community-based method against the retrospective FBH/FPH for rolling twelve-month periods. For each method we calculated total cost, average annual cost per 1,000 population, and average cost per vital event reported.
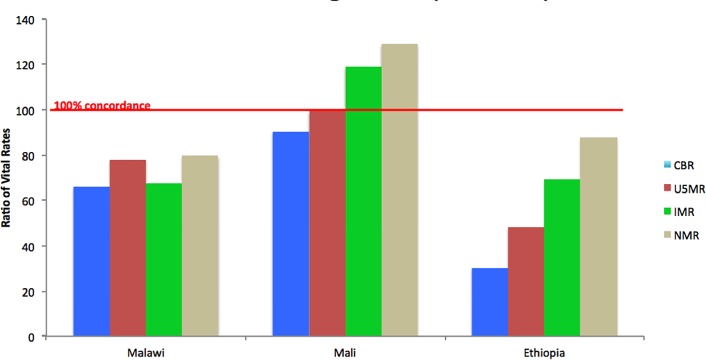
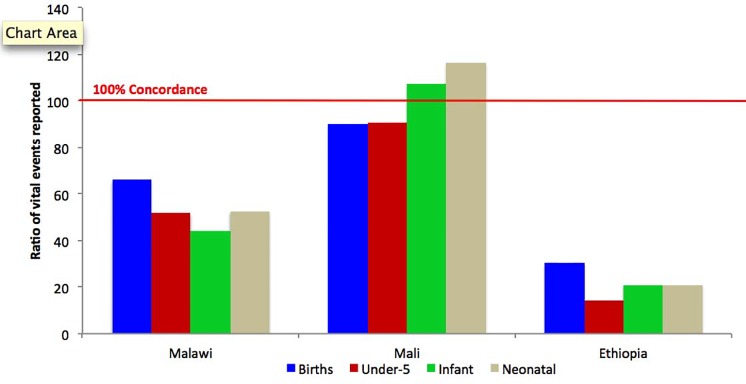
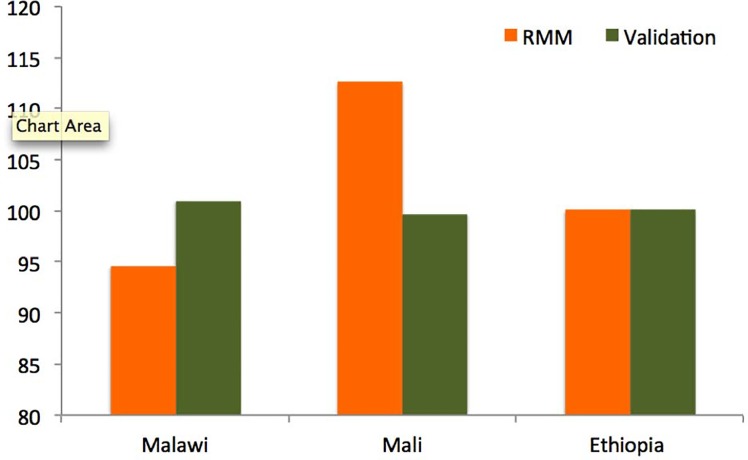
On average, CHWs submitted monthly vital event reports for over 95 percent of catchment areas in Ethiopia and Malawi, and for 100 percent of catchment areas in Mali. The completeness of vital events reporting by CHWs varied: we estimated that 30%-90% of annualized expected births (i.e. the number of births estimated using a FPH) were documented by CHWs and 22%-91% of annualized expected under-five deaths were documented by CHWs. Resulting annualized under-five mortality rates based on the CHW vital events reporting were, on average, under-estimated by 28% in Ethiopia, 32% in Malawi, and 9% in Mali relative to comparable FPHs. Costs per vital event reported ranged from $21 in Malawi to $149 in Mali.
Our findings in Mali suggest that CHWs can collect complete and high-quality vital events data useful for monitoring annual changes in under-five mortality rates. Both the supervision of CHWs in Mali and the rigor of the associated field-based data quality checks were of a high standard, and the size of the pilot area in Mali was small (comprising of approximately 53,205 residents in 4,200 households). Hence, there are remaining questions about whether this level of vital events reporting completeness and data quality could be maintained if the approach was implemented at scale. Our experience in Malawi and Ethiopia suggests that, in some settings, establishing and maintaining the completeness and quality of vital events reporting by CHWs over time is challenging. In this sense, our evaluation in Mali falls closer to that of an efficacy study, whereas our evaluations in Ethiopia and Malawi are more akin to an effectiveness study. Our overall findings suggest that no one-size-fits-all approach will be successful in guaranteeing complete and accurate reporting of vital events by CHWs.
大多数低收入国家缺乏完整且准确的人口动态登记系统。因此,五岁以下儿童死亡率的衡量主要依赖于家庭调查。我们与埃塞俄比亚、加纳、马拉维和马里的合作伙伴合作,评估了社区卫生工作者报告出生和死亡情况的完整性与准确性,以及根据这些数据得出的五岁以下儿童死亡率年度估计值的准确性。在此,我们报告埃塞俄比亚、马拉维和马里的结果。
在这三个国家,社区卫生工作者均接受了培训、配备了设备并获得支持,以便在至少十五个月的时间内报告特定地理区域内的怀孕、出生和死亡情况。各国国内机构每月收集这些数据。在每个研究地点,我们通过在马里进行的家庭普查以及在埃塞俄比亚和马拉维进行的家庭调查,向育龄妇女询问完整的生育史(FBH)或完整的怀孕史(FPH)。以这些FBH/FPH作为验证数据源,我们评估了基于社区方法得出的出生和死亡计数的完整性,以及滚动十二个月期间五岁以下、婴儿和新生儿死亡率相对于回顾性FBH/FPH的准确性。对于每种方法,我们计算了总成本、每千人口的年均成本以及报告的每起重要事件的平均成本。
平均而言,社区卫生工作者为埃塞俄比亚和马拉维超过95%的集水区提交了月度重要事件报告,为马里100%的集水区提交了报告。社区卫生工作者报告重要事件的完整性各不相同:我们估计,社区卫生工作者记录了30%-90%的年度预期出生数(即使用FPH估计的出生数)以及22%-91%的年度预期五岁以下儿童死亡数。基于社区卫生工作者报告的重要事件得出的五岁以下儿童死亡率年度估计值,相对于可比的FPH,在埃塞俄比亚平均低报28%,在马拉维低报32%,在马里低报9%。报告的每起重要事件的成本从马拉维的21美元到马里的149美元不等。
我们在马里的研究结果表明,社区卫生工作者能够收集完整且高质量的重要事件数据,这些数据有助于监测五岁以下儿童死亡率的年度变化。马里对社区卫生工作者的监督以及相关实地数据质量检查的严格程度都很高,而且马里试点地区的规模较小(由4200户家庭中的约53205名居民组成)。因此,如果该方法大规模实施,能否维持这种重要事件报告的完整性和数据质量水平仍存在疑问。我们在马拉维和埃塞俄比亚的经验表明,在某些情况下,随着时间的推移建立并维持社区卫生工作者报告重要事件的完整性和质量具有挑战性。从这个意义上说,我们在马里的评估更接近于一项效能研究,而我们在埃塞俄比亚和马拉维的评估更类似于一项效果研究。我们的总体研究结果表明,没有一种通用方法能成功保证社区卫生工作者完整准确地报告重要事件。