Research Division, LVCT Health, PO Box 19835-00202, Nairobi, Kenya.
REACH Trust, Box 1597, Lilongwe, Malawi.
Health Policy Plan. 2020 Apr 1;35(3):334-345. doi: 10.1093/heapol/czz163.
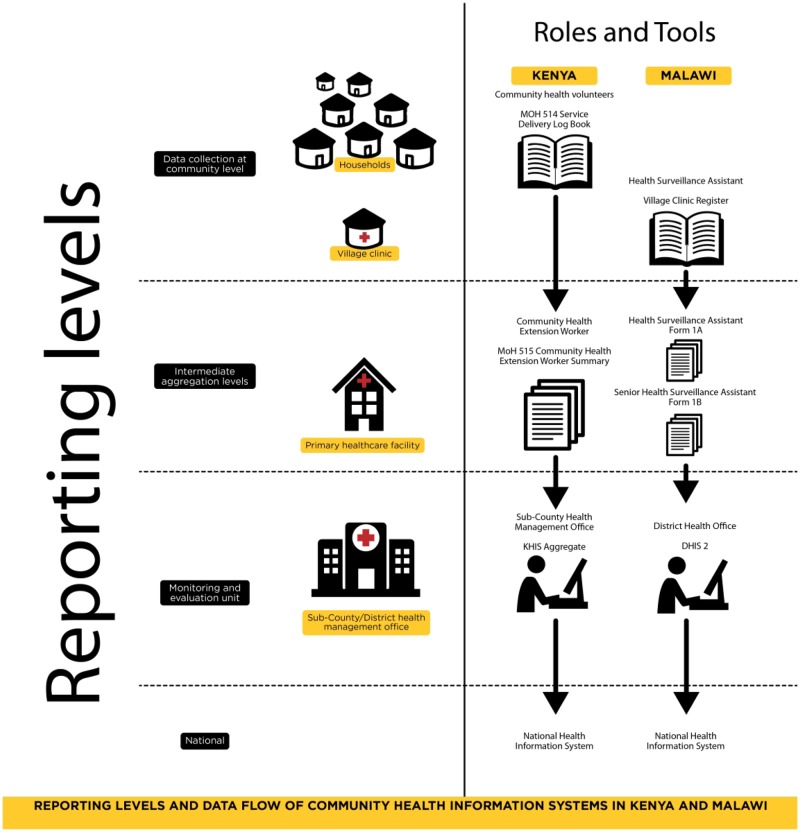
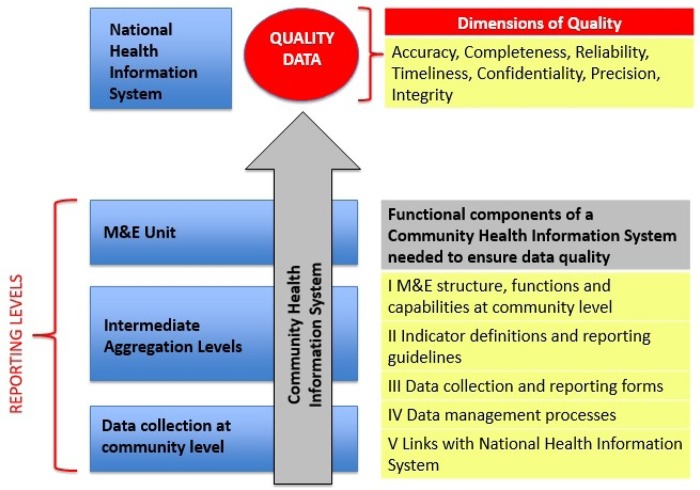
High-quality data are essential to monitor and evaluate community health worker (CHW) programmes in low- and middle-income countries striving towards universal health coverage. This mixed-methods study was conducted in two purposively selected districts in Kenya (where volunteers collect data) and two in Malawi (where health surveillance assistants are a paid cadre). We calculated data verification ratios to quantify reporting consistency for selected health indicators over 3 months across 339 registers and 72 summary reports. These indicators are related to antenatal care, skilled delivery, immunization, growth monitoring and nutrition in Kenya; new cases, danger signs, drug stock-outs and under-five mortality in Malawi. We used qualitative methods to explore perceptions of data quality with 52 CHWs in Kenya, 83 CHWs in Malawi and 36 key informants. We analysed these data using a framework approach assisted by NVivo11. We found that only 15% of data were reported consistently between CHWs and their supervisors in both contexts. We found remarkable similarities in our qualitative data in Kenya and Malawi. Barriers to data quality mirrored those previously reported elsewhere including unavailability of data collection and reporting tools; inadequate training and supervision; lack of quality control mechanisms; and inadequate register completion. In addition, we found that CHWs experienced tensions at the interface between the formal health system and the communities they served, mediated by the social and cultural expectations of their role. These issues affected data quality in both contexts with reports of difficulties in negotiating gender norms leading to skipping sensitive questions when completing registers; fabrication of data; lack of trust in the data; and limited use of data for decision-making. While routine systems need strengthening, these more nuanced issues also need addressing. This is backed up by our finding of the high value placed on supportive supervision as an enabler of data quality.
高质量的数据对于监测和评估努力实现全民健康覆盖的中低收入国家的社区卫生工作者(CHW)计划至关重要。本混合方法研究在肯尼亚的两个有针对性选择的地区(志愿者收集数据)和马拉维的两个地区(卫生监测助理是有薪干部)进行。我们计算了数据验证比,以量化在 339 个登记簿和 72 份汇总报告中,3 个月内选定健康指标的报告一致性。这些指标与肯尼亚的产前护理、熟练分娩、免疫、生长监测和营养有关;马拉维的新病例、危险迹象、药物缺货和五岁以下儿童死亡率。我们使用定性方法探讨了 52 名肯尼亚 CHW、83 名马拉维 CHW 和 36 名关键信息提供者对数据质量的看法。我们使用框架方法分析了这些数据,并使用 NVivo11 提供帮助。我们发现,在这两个地区,只有 15%的数据在 CHW 和他们的主管之间一致报告。我们在肯尼亚和马拉维的定性数据中发现了惊人的相似之处。数据质量的障碍与其他地方报告的障碍相似,包括数据收集和报告工具不可用;培训和监督不足;缺乏质量控制机制;以及登记簿填写不充分。此外,我们发现 CHW 在正式卫生系统和他们服务的社区之间的界面上存在紧张关系,这是由他们角色的社会和文化期望介导的。这些问题在两个地区都影响了数据质量,报告称在填写登记簿时,难以协商性别规范导致跳过敏感问题;数据捏造;对数据缺乏信任;以及数据在决策中的有限使用。虽然常规系统需要加强,但这些更细微的问题也需要解决。这得到了我们的发现的支持,即支持性监督被认为是提高数据质量的一个手段。